
What "Comfort-Focused Care" Really Means — and When to Ask About It
Families across Monterey County hear the phrase "comfort-focused care" at some point during a serious illness — often from a doctor, a discharge planner at Community Hospital of the Monterey Peninsula, or a nurse after a difficult diagnosis. And most of the time, they nod along without being entirely sure what it means.
That's not their fault. The phrase gets used loosely, and it carries emotional weight that makes people hesitant to ask follow-up questions. Does it mean treatment is stopping? Does it mean the end is near? Does choosing comfort mean giving up?
The honest answers are no, not necessarily, and never. What comfort-focused care actually describes is a shift in what the care team is working toward — and understanding that shift is one of the most useful things a family can know when they're navigating serious illness.
The Difference Between Curing and Caring
Most of the medical system is built around fixing things — treating infections, removing tumors, repairing damage. That approach works well when the problem is solvable. But for many people living with a serious or advanced illness, cure isn't always on the table. And that's when the goals of care need to shift.
Comfort-focused care means the primary goal becomes quality of life — not length of life, not test results, not disease management for its own sake. It asks: what does this person need to feel as well as possible, right now, in the life they're actually living?
For a 78-year-old in Salinas managing congestive heart failure, that might mean adjusting medications to reduce breathlessness rather than pursuing another hospitalization. For someone in Pacific Grove with advanced cancer, it might mean focusing on pain control, sleep, and being present with family rather than continuing chemotherapy with significant side effects.
This isn't a lesser form of care. In many cases it requires more clinical attention, not less — because managing complex symptoms at home takes real skill. What does a skilled nurse actually do on a home visit? is a question worth asking, because the answer might surprise families who assume comfort care is just "keeping someone comfortable" in a passive sense.
Palliative Care vs. Hospice — Where Comfort Care Lives
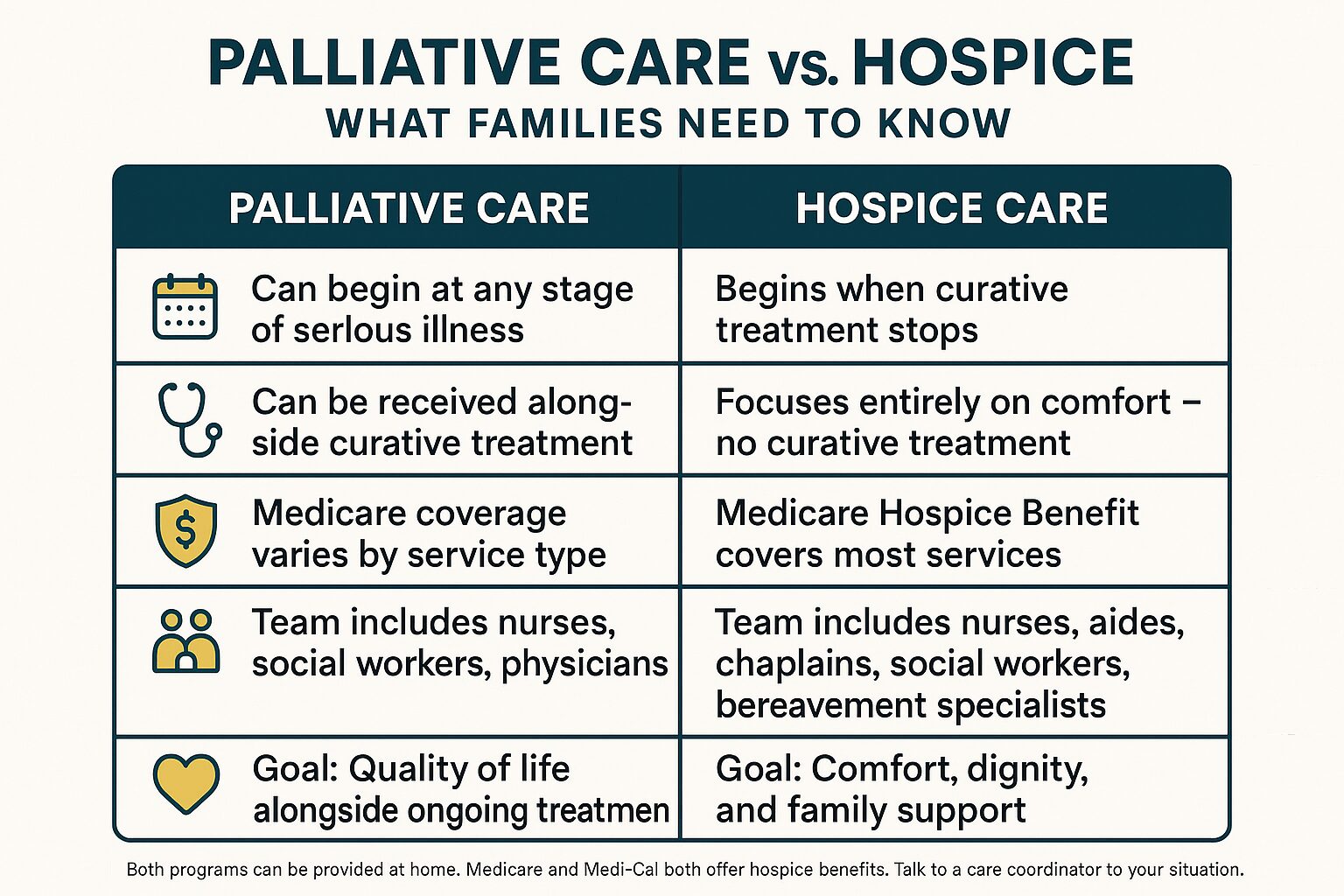
Two programs put comfort-focused care into practice: palliative care and hospice. They're related, but they're not the same thing, and the difference matters a lot to families trying to make decisions.
Palliative care can start at any point after a serious diagnosis — even while a person is still pursuing curative treatment. It layers on top of whatever else is happening medically. A person can be receiving chemotherapy and palliative care at the same time. The palliative care team focuses on symptoms, emotional support, care planning, and helping the family understand what's ahead.
Hospice care is specifically for people who have decided — usually alongside their physician — to stop pursuing curative treatment and focus entirely on comfort. Medicare's hospice benefit requires a physician to certify that the patient's life expectancy is six months or less if the illness follows its expected course. But it's important to know: people can live on hospice longer than six months, and they can also choose to leave hospice if their condition stabilizes.
Here's how families often describe the distinction:
- Palliative care: still fighting the illness, but with a team helping manage the burden of it
- Hospice care: no longer trying to cure the illness, with a team focused entirely on comfort and quality of life
Both involve nurses, therapists, social workers, chaplains, and volunteers working together. Neither one is about doing less. For a deeper look at what palliative care actually means for families, it's worth reading through the specifics before making any decisions.

Palliative Care vs. Hospice: A Side-by-Side Look
This comparison helps families quickly see how the two programs differ in terms of goals, timing, and what Medicare covers.
When Families Actually Ask About It — and Why They Wait
In Monterey County, families often ask about comfort-focused care later than they wish they had. This comes up again and again — not because families don't care, but because the system doesn't always make it easy to know when to bring it up.
There's no single right moment. But there are signals worth paying attention to:
- A loved one has been hospitalized two or more times in the past six months for the same condition
- Treatments are causing significant side effects without clear benefit
- A physician has mentioned that the illness is "not responding" or is "progressing"
- The person with the illness has expressed that they feel tired of treatment
- A family member has had to step back from work or their own life to manage care
- Discharge planners at the hospital have raised the question of home-based support
None of these signals means hospice is the immediate answer. But they do mean the conversation is worth having. What families in Monterey wish they'd known sooner about home care often includes wishing they had asked about comfort-focused options earlier — not because it would have changed the outcome, but because it would have reduced suffering in the meantime.
And asking doesn't commit anyone to anything. It's a conversation, not a contract.
What Comfort-Focused Care Can Look Like at Home
Comfort-focused care is practical, not abstract. Here's a plain-language look at what different team members actually do in the home.
| Team Member | What They Focus On | How Often They Visit |
|---|---|---|
| Registered Nurse (RN) | Pain assessment, medication management, wound care, symptom monitoring | Several times per week, or as needed |
| Licensed Vocational Nurse (LVN) | Medication review, vital signs, day-to-day symptom support | Coordinated with RN schedule |
| Medical Social Worker | Emotional support, care planning, connecting families to local resources | Weekly or as needed |
| Chaplain | Spiritual care and emotional presence for patient and family | As requested or scheduled |
| Hospice Aide | Personal care, bathing, comfort routines | Daily or several times per week |
| Bereavement Specialist | Grief support for family members — before and after the patient's passing | Ongoing, continues after death |
| Volunteers | Companionship, respite for family, errands, reading aloud | Flexible, scheduled with the family |
How Medicare and Medi-Cal Actually Cover This
One of the biggest reasons families hesitate to ask about comfort-focused care is cost. The assumption is that it's expensive, or that insurance won't cover it. In most cases, that assumption is wrong.
Medicare's Hospice Benefit covers virtually all hospice-related services for eligible patients — nursing visits, medications related to the terminal diagnosis, medical equipment like hospital beds and wheelchairs, and support from the full care team including chaplains and bereavement specialists. The patient typically pays nothing out of pocket for these services.
Medi-Cal also provides a hospice benefit with similar coverage. And for veterans living in Salinas, King City, Hollister, or elsewhere in the region, VA benefits may cover home-based comfort care as well.
Palliative care coverage is more variable. It depends on the specific services and how they're billed. But many palliative care visits — particularly those involving Registered Nurses or social workers — are covered under standard Medicare home health benefits when a physician orders them.
If you're uncertain what would be covered in a specific situation, a care coordinator can walk through the details before any commitment is made. What families need to know about Medicare coverage for home care covers many of the common questions families ask.
Frequently Asked Questions About Comfort-Focused Care
Does choosing comfort-focused care mean we're giving up?
No. Choosing comfort-focused care means changing the goal — from trying to cure an illness to making sure the person with that illness feels as well as possible. Many families who've made that shift say it was the most loving decision they ever made, not a defeat. How families describe the moment they chose hospice is worth reading if you're wrestling with this question.
Can someone receive palliative care while still getting chemotherapy or other treatment?
Yes. Palliative care does not require stopping treatment. It works alongside whatever treatment a person is receiving. The palliative care team focuses on managing symptoms — nausea, pain, fatigue, anxiety — that treatment often causes, as well as supporting the family through a difficult time.
What happens if someone on hospice starts to get better?
They can leave hospice. There's no penalty and no paperwork punishment for choosing to resume curative treatment if a person's condition improves. Some people stabilize, leave hospice, and re-enroll later. The hospice benefit under Medicare can be used more than once.
How do we know if our family member qualifies for hospice?
Qualification requires a physician to certify that the patient's life expectancy is six months or less if the illness follows its expected path. The patient (or their representative) also needs to agree to focus on comfort rather than cure. A care coordinator or the patient's physician can help determine eligibility — it's a conversation, not a complicated application process.
Can comfort-focused care happen at home, or does it require a facility?
Most comfort-focused care — including both palliative care and hospice — is delivered at home. For families in Monterey County, that means a patient can stay in their own house, with their own routines and the people they love around them, while still receiving skilled clinical support. Facility-based hospice exists but is typically reserved for symptom crises that can't be managed at home.
What support does the family get — not just the patient?
Quite a bit. Hospice care includes medical social workers for emotional and practical support, chaplains for spiritual care, and bereavement specialists who work with the family both before and after a patient's passing. Bereavement support continues for at least 13 months after the death of a loved one under the Medicare Hospice Benefit. That's not a minor detail — grief doesn't follow a schedule, and having a bereavement specialist available during that time makes a real difference.
Still Have Questions About What This Could Look Like for Your Family?
Central Coast VNA & Hospice has been supporting families across Monterey County — from the Peninsula to Salinas to King City — since 1951. If you're trying to understand whether comfort-focused care makes sense for your situation, a care coordinator can talk through the specifics without pressure or obligation. Call 831-372-6668 or visit ccvna.com to start the conversation.
How Families Describe the Moment They Chose Hospice
Most people don't know what the moment of choosing hospice feels like until they're in it. There's no manual for it, no checklist that makes it easy, and no way to fully prepare for what it asks of a family.
Across Monterey County — from Pacific Grove to Salinas to King City — families have sat in living rooms and hospital waiting areas and made this decision while exhausted, grieving, and scared. What they describe afterward is almost never what they expected.
This article is about those real experiences: what pushed families to finally ask about hospice, what surprised them when they did, and what they most wish they had known before the conversation started.
The Moment Families Say Everything Changed
When families talk about choosing hospice, they rarely describe a single dramatic turning point. More often, it's a slow accumulation — weeks of hospitalizations, a loved one who stopped eating, a treatment that wasn't working and everyone quietly knew it.
Then something tips the scale. A doctor says the words "there's nothing more we can do to cure this." Or a parent looks at their child and says, "I just want to go home."
For many families in Monterey County, the conversation started not in a hospital room but at home, when a nurse or physician finally said what the family had been feeling but hadn't said out loud: that continuing aggressive treatment might be causing more suffering than it was preventing.
What families describe most consistently is relief — not happiness, not closure, but relief. The relief of finally having a direction. The relief of knowing that comfort and dignity were now the whole focus, not a secondary concern.
Some families also describe guilt in that same moment. Guilt that they weren't fighting harder. Guilt that it might look to others like they were giving up. One of the most important things families later say is that they wish someone had told them sooner: choosing hospice is not giving up on a person. It's choosing to be fully present with them.
If you're still weighing options and wondering when the right time is, what families in Monterey wish they'd known sooner about home care covers some of that ground in plain terms.
What Families Didn't Expect When Hospice Care Started
Almost every family says the same thing: "We should have done this sooner."
That's not a small thing to say. These are people who spent months in hospitals and treatment centers doing everything they could. And then hospice started, and something shifted in the house.
Here's what families across the Central Coast have described after hospice care began:
- The pain was finally managed. For many patients, hospice was the first time their pain was consistently addressed — not treated as a side issue, but as the main priority.
- Someone was actually available. The hospice team — including nurses, Medical Social Workers, Chaplains, and Volunteers — came to them. The family wasn't driving to appointments or navigating a phone tree at 2 a.m.
- Their loved one became more present. When pain and anxiety are managed, people often become more themselves again. Families describe conversations they didn't think were possible anymore.
- They were part of the care. Hospice didn't push families to the side. It included them — walking them through medications, explaining what was happening, preparing them for what was coming.
The interdisciplinary team matters more than most families expect going in. Registered Nurses and Licensed Vocational Nurses manage symptoms and medications. Physical Therapists and Occupational Therapists help patients stay as mobile and comfortable as possible. Chaplains support spiritual needs — regardless of faith background. Bereavement Specialists begin supporting families before the death, not just after.
For a closer look at what a skilled nurse actually does on a visit, this guide breaks it down in real terms.
Hospice vs. Continued Treatment: What Families Were Weighing
This isn't a clinical comparison — it's a reflection of the real questions families describe wrestling with before they made their decision.
| What Families Were Asking | Continued Treatment Path | Hospice Care Path |
|---|---|---|
| Where will my loved one be? | Hospital, clinic, or facility visits | At home, wherever home is |
| What's the main goal? | Slow or stop disease progression | Comfort, dignity, quality of life |
| Who manages day-to-day care? | Rotating hospital or clinic staff | A consistent team of nurses, therapists, social workers, chaplains |
| What about pain management? | Often secondary to treatment goals | The primary focus from day one |
| Is Medicare involved? | Covered under standard Medicare benefits | Covered under the Medicare Hospice Benefit — typically $0 out of pocket for eligible patients |
| When does support for family start? | Mostly after the patient's death | During care — and continues for at least 13 months after loss through bereavement services |
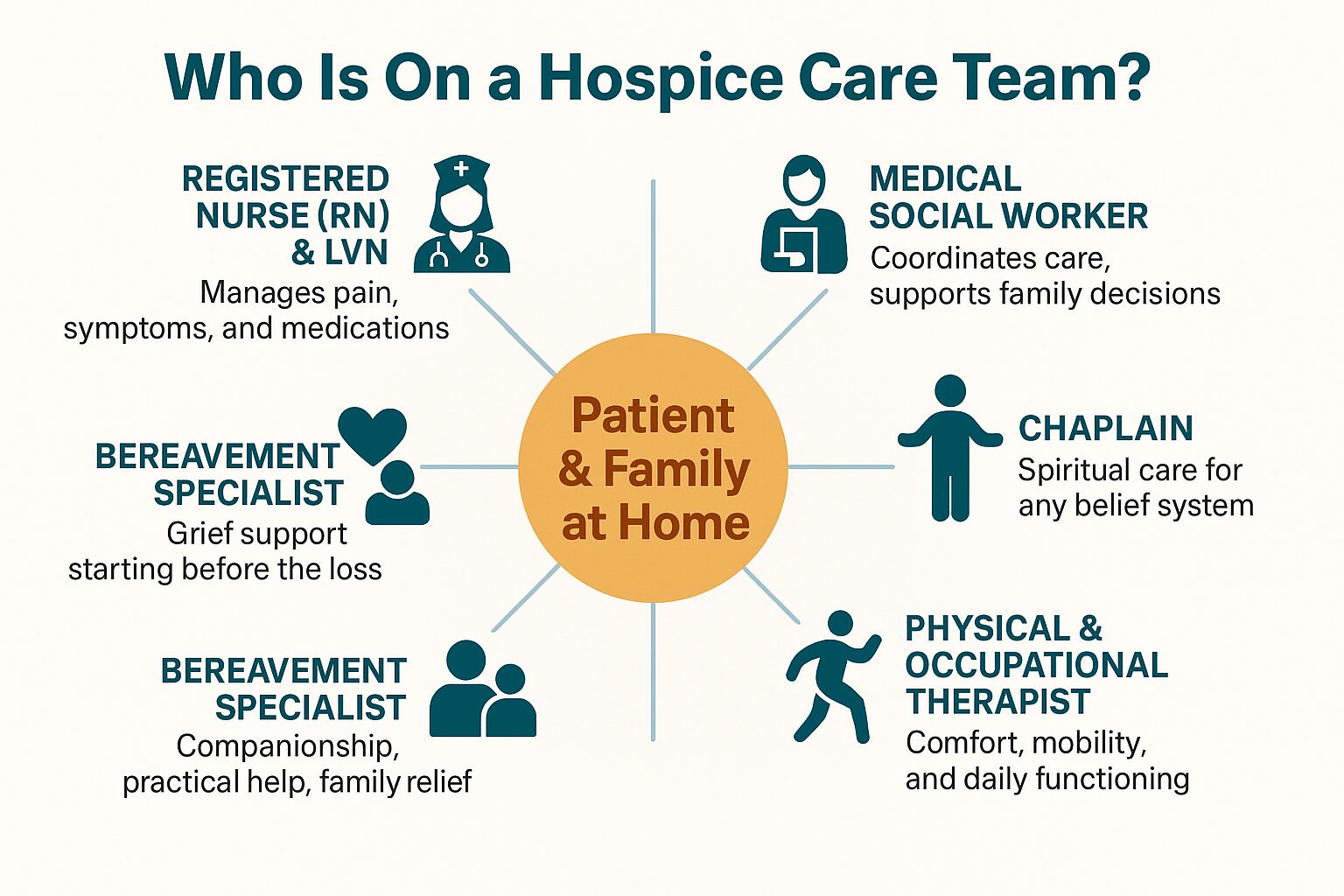
The Hospice Team: Who's in the Room (and Why It Matters)
Families often don't realize how many people are involved in hospice care until it starts. This shows the full team and what each person actually does.
The Question Families Wish They Had Asked Earlier
The single most common thing families say — across Monterey, Salinas, Hollister, and every other community in this region — is a version of the same sentence: "Why did we wait so long?"
There's a widespread belief that asking about hospice means you're ready to give up, that it's only for the final days of life. But Medicare's hospice benefit is available when a physician certifies that a patient's illness, if it follows its expected course, may limit life expectancy to six months or less. That's not days. That's months — months that could be spent at home, comfortable, surrounded by people who matter.
Many families in Monterey County also don't realize that hospice doesn't require giving up all treatment. Patients can continue medications that manage their condition. What changes is the goal: treatment shifts from trying to cure the illness to managing symptoms and supporting quality of life.
If your family is somewhere in between — not ready for hospice but aware that a serious illness is changing things — palliative care is worth understanding. It supports comfort and care planning alongside whatever treatment is already happening, without requiring a hospice election.
And for families still trying to understand when any kind of additional support makes sense, this guide on when it's time to think about getting help at home covers the early warning signs in plain language.
What Grief Looks Like After — and Why Support Doesn't Stop
Families who choose hospice don't just lose a loved one. They lose the role they'd been playing — the coordinator, the advocate, the person managing every appointment and medication.
Grief after hospice often surprises people. Some families feel relief and then feel guilty about the relief. Others feel the loss more acutely weeks or months later, after the caregiving structure falls away.
Hospice bereavement services exist specifically for this. Under the Medicare Hospice Benefit, bereavement support is required for at least 13 months following a patient's death. That includes regular contact from Bereavement Specialists, grief counseling, and community resources — not just a single follow-up call.
For families in Monterey County, this ongoing support is part of what makes the hospice experience different from what most people expect going in. The team that helped at the end doesn't simply disappear. To understand more about what grief support looks like after a loss, this guide to bereavement counseling explains what's available and how to access it.
Frequently Asked Questions About Choosing Hospice
Does choosing hospice mean we're giving up on our loved one?
That's the fear almost every family carries into the conversation. But what families consistently describe afterward is that hospice felt like the opposite of giving up — it meant committing fully to the person's comfort, dignity, and quality of life. The goal shifts from fighting the disease to being fully present. That's not surrender. That's a different kind of fight.
When is the right time to ask about hospice?
Earlier than most families think. Medicare's hospice benefit becomes available when a physician certifies that an illness may limit life expectancy to six months or less if it follows its expected course. Many families wait until the final days — and later say that was their biggest regret. If serious illness is changing your loved one's daily life, asking the question now doesn't commit you to anything. It just gives you information.
What does hospice cost for families in Monterey County?
For patients covered by Medicare or Medi-Cal, hospice care is typically covered at $0 out of pocket — including nursing visits, medications related to the terminal diagnosis, equipment, and the full interdisciplinary team. Veterans benefits also cover hospice for qualifying patients. Cost is rarely the barrier families expect it to be.
Can my loved one leave hospice if things improve?
Yes. Hospice is not a one-way door. If a patient's condition stabilizes or improves, they can be discharged from hospice and return to curative treatment. They can also re-enroll later if needed. The decision is always in the hands of the patient and family.
What happens to our family after our loved one passes?
Bereavement support continues for at least 13 months after the death. Bereavement Specialists stay in contact with families, provide grief counseling, and connect families with community resources. The care doesn't end when the patient dies.
Is there a difference between hospice and palliative care?
Yes, and it matters. Palliative care can happen alongside any treatment, at any stage of serious illness — it's focused on comfort, symptom management, and care planning, without requiring patients to give up curative care. Hospice is a specific program for patients who have decided to focus entirely on comfort rather than treatment. Many families move from palliative care to hospice as illness progresses.
Ready to Have the Conversation?
If you're somewhere in the middle of this — not sure if it's time, not sure what to ask, not sure how your loved one will respond — that's exactly where most families are when they first call. Central Coast VNA & Hospice has been serving families across Monterey County, Salinas, Hollister, and the surrounding Central Coast since 1951, and the first conversation doesn't commit anyone to anything. You can reach a care coordinator at 831-372-6668, or learn more at ccvna.com.

After the Hospital Discharge, What Comes Next?
The discharge papers are signed. Your parent or spouse is being wheeled to the car. And now you're thinking: what exactly happens next?
For families across Monterey County — whether you're driving home from Community Hospital of the Monterey Peninsula in Monterey or Natividad Medical Center in Salinas — that moment can feel disorienting. The hospital felt safe. Home feels like a question mark.
Most patients are actually better served at home than in a skilled nursing facility after discharge, especially with the right support in place. This article walks you through what that transition really looks like, what Medicare typically covers, and how to tell whether your loved one's needs can be met at home.
What 'Discharge Planning' Actually Means — and Why It Matters
Hospitals are required to have a discharge plan in place before a patient leaves. But in practice, families often receive that plan hours before departure — sometimes as a stack of papers, sometimes as a rushed hallway conversation with a social worker.
A discharge plan typically includes:
- A summary of the patient's diagnosis and treatment
- A medication list, often with recent changes
- Follow-up appointment instructions
- Referrals to home health services, if ordered by the physician
- Activity restrictions and wound care instructions, if applicable
The most important thing to understand is this: a physician must order home health services. If the discharging doctor didn't bring it up and you believe your loved one needs skilled care at home, you can — and should — ask directly before leaving the hospital.
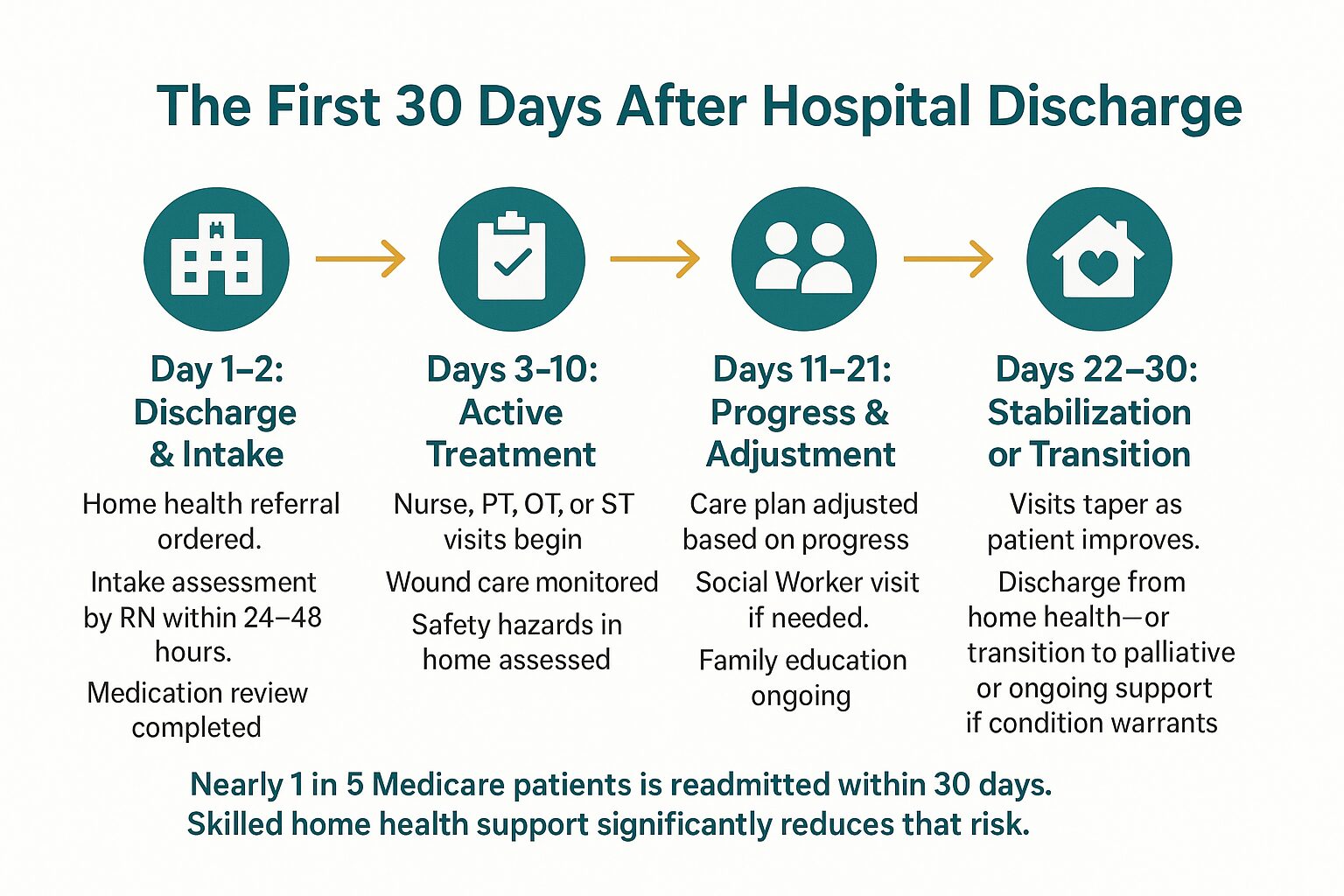
If a home health referral is in the plan, services can often begin within 24 to 48 hours of discharge. That window matters, because the first few days at home carry the highest risk of readmission. According to Medicare data, nearly 1 in 5 Medicare patients is readmitted within 30 days of hospital discharge — most often due to medication errors, missed follow-up, or inadequate wound care monitoring at home.
Understanding what a skilled nurse actually does on a home visit can help families know exactly what to expect from those first days.

What Home Health Services Look Like in the First Weeks
Once home health is ordered, an intake assessment happens first — usually within 24 hours of the referral. A Registered Nurse or Licensed Vocational Nurse visits the home, reviews the discharge summary, assesses the patient's condition, and develops a care plan with the treating physician.
Depending on what the patient needs, the care team may include:
- Registered Nurses (RNs) and Licensed Vocational Nurses (LVNs) for wound care, medication management, and health monitoring
- Physical Therapists for rebuilding strength and mobility after surgery or a fall
- Occupational Therapists to help patients safely perform daily tasks — bathing, dressing, cooking — in their own home
- Speech Therapists if swallowing, speech, or cognitive function was affected
- Medical Social Workers to help with care planning, community resources, and family support
Visit frequency depends on clinical need, not a fixed schedule. Someone recovering from hip replacement surgery in Salinas might have a Physical Therapist and RN visiting three to five days per week in the first two weeks, then tapering as they improve.
One thing families sometimes don't expect: home health is episodic care, not ongoing custodial support. Clinicians come to assess, treat, and teach — not to provide daily personal care or companionship. If your family is sorting through what level of help is actually needed, the difference between needing help and needing a facility lays that out clearly.
Common Needs After Discharge — Who Addresses Them
Families often don't know which type of clinician handles which post-discharge need. This table gives a quick reference for the most common situations.
| Post-Discharge Need | Who Addresses It | Typical Frequency |
|---|---|---|
| Wound care and surgical site monitoring | Registered Nurse (RN) or LVN | 2–5 visits/week initially |
| Medication changes and safety review | Registered Nurse (RN) | First visit, then as needed |
| Walking, balance, and strength recovery | Physical Therapist (PT) | 2–4 visits/week |
| Safe return to daily activities at home | Occupational Therapist (OT) | 1–3 visits/week |
| Swallowing or speech difficulty post-stroke | Speech Therapist (ST) | 2–3 visits/week |
| Care coordination, family support, resource navigation | Medical Social Worker | 1–2 visits total, or as needed |
| Pain and symptom management for serious illness | RN + full interdisciplinary team | Varies by care plan |
The First 30 Days at Home: What a Typical Recovery Path Looks Like
The 30 days after hospital discharge are the highest-risk window for readmission. This infographic maps out what a supported recovery typically looks like week by week.
What Medicare Covers — and Where Families Get Confused
Medicare Part A and Part B both cover home health services, but the rules trip people up. The most common misconceptions families in Monterey County run into:
Myth: Medicare only pays if you were hospitalized first.
Not true. Medicare covers home health services as long as a physician certifies that the patient is homebound and needs skilled care — regardless of whether there was a recent hospitalization.
Myth: Medicare pays for 24-hour home care.
It doesn't. Medicare covers skilled, intermittent care — meaning clinician visits, not round-the-clock supervision or personal care assistance.
What Medicare does cover:
- Skilled nursing visits (RN or LVN)
- Physical, occupational, and speech therapy
- Medical Social Worker services
- Home health aide visits when skilled care is also being received
- Medical supplies related to the plan of care
There is no copay for Medicare-covered home health services when the agency is Medicare-certified. Families eligible for Medi-Cal may have additional benefits that cover services Medicare doesn't reach. Veterans may have separate coverage through the VA.
For a fuller breakdown of how coverage works when Medicare doesn't cover everything, this guide walks through your options. And if physical therapy is part of the picture, Medicare's coverage of home physical therapy is worth reading before discharge day.
When Home Health Isn't Enough — What Comes After
For most patients recovering from surgery or an acute illness, home health is a temporary bridge. They improve, visits taper off, and they return to managing life independently.
But for patients with a serious or progressive illness — someone with advanced heart failure, COPD, or cancer — discharge may mark the beginning of a longer road. That's where families need to know the difference between home health, palliative care, and hospice, because these are not the same thing.
Palliative care is specialized support for serious illness that can run alongside any other treatment. It focuses on symptom management, care planning, and emotional support for both the patient and family — and patients do not have to give up curative treatment to receive it. If your family is trying to understand what this actually looks like in practice, this guide to palliative care meaning and family support is a useful starting point.
Hospice care is for patients whose illness has progressed to a point where treatment is no longer the focus — where comfort, dignity, and quality of life at home become the priority. It includes a full team: nurses, therapists, social workers, chaplains, volunteers, and bereavement specialists who support the entire family. If you're wondering whether that conversation is worth having, The Heart of Hospice: A Guide for Families explains it without pressure.
For many families in Salinas, King City, Hollister, and across Monterey County, the question isn't whether to ask — it's finding a trustworthy place to start.
Frequently Asked Questions About Home Care After Hospital Discharge
How quickly can home health services start after my parent is discharged?
In most cases, an intake visit from a Registered Nurse can happen within 24 to 48 hours of discharge. If the referral is sent from the hospital before discharge, the timeline can be even shorter. The key is making sure the discharging physician submits the order before your loved one leaves the facility.
My dad was only in the hospital for two days. Does he still qualify for home health?
Possibly, yes. Medicare's home health benefit doesn't require a minimum hospital stay — it requires that a physician certify the patient as homebound and in need of skilled care. A two-day stay for a cardiac event or fall, for example, can absolutely qualify someone for post-discharge home nursing or therapy.
What does 'homebound' mean for Medicare purposes?
It means that leaving home requires a considerable effort and is medically inadvisable or physically difficult. A patient who can walk to the mailbox but cannot safely drive or travel without help typically qualifies. Your Registered Nurse or the intake team can help assess this during the first visit.
We live in King City — can home health actually reach us?
Yes. Service extends throughout Monterey County, including King City and the South County communities. Distance from the Monterey Peninsula doesn't disqualify a patient from receiving home health, though scheduling and visit frequency may look slightly different in more rural areas.
What if my family needs more support than skilled visits can provide?
Skilled home health focuses on medical and therapeutic care, not daily personal assistance or companionship. If your loved one needs help with bathing, meals, or daily supervision beyond what clinicians provide, a Medical Social Worker can help identify community resources and non-medical support options available in Monterey County. That conversation is worth having early — not after a crisis.
Is there any cost to the family for home health under Medicare?
No copay for Medicare-covered home health services when you're using a Medicare-certified agency. The services covered — skilled nursing, therapy, social work, home health aide visits — come at no out-of-pocket cost to Medicare beneficiaries who meet the eligibility criteria.
Questions About What Comes Next for Your Family?
Central Coast VNA & Hospice has been supporting families through exactly this kind of transition since 1951 — across Monterey County, from the Peninsula to Salinas to King City and beyond. If you're trying to sort out what your loved one qualifies for, what Medicare covers, or whether home health is the right fit, a care coordinator can talk it through with you without pressure. Call 831-372-6668 or visit ccvna.com to start that conversation.
What Does a Skilled Nurse Actually Do on a Home Visit?
Most families in Monterey County have a vague sense that home nursing means 'someone comes to check on Mom.' But when you're making real decisions about a parent recovering from surgery in Pacific Grove or managing heart failure in Salinas, 'someone checks in' doesn't tell you much.
A skilled nursing visit is a medical appointment — it just happens in your living room instead of a clinic. The nurse arrives with clinical tools, a care plan, and direct communication with your loved one's physician. What they do in that hour or so has real consequences for whether someone stays stable at home or ends up back in the hospital.
This article walks through what actually happens during those visits, what problems skilled nurses are trained to catch, and how to know whether your family's situation fits what home health can provide.
The First Visit: More Than a Checkup
The initial home visit is longer and more detailed than follow-up visits — often 60 to 90 minutes. A Registered Nurse conducts a head-to-toe assessment that covers far more than vital signs.
They're building a clinical picture of the patient in their actual environment. That means looking at how the person moves through their home, whether they can safely take their own medications, and what the home itself might be doing to their health — poor lighting, loose rugs, a second-floor bathroom when someone has balance problems.
For families in Monterey County, that first visit also establishes a baseline. If your parent was discharged from Salinas Valley Health or Community Hospital of the Monterey Peninsula after a hip replacement, the nurse arriving at home is working from that discharge summary and confirming that what was documented actually matches what they see in front of them. Those details don't always line up.
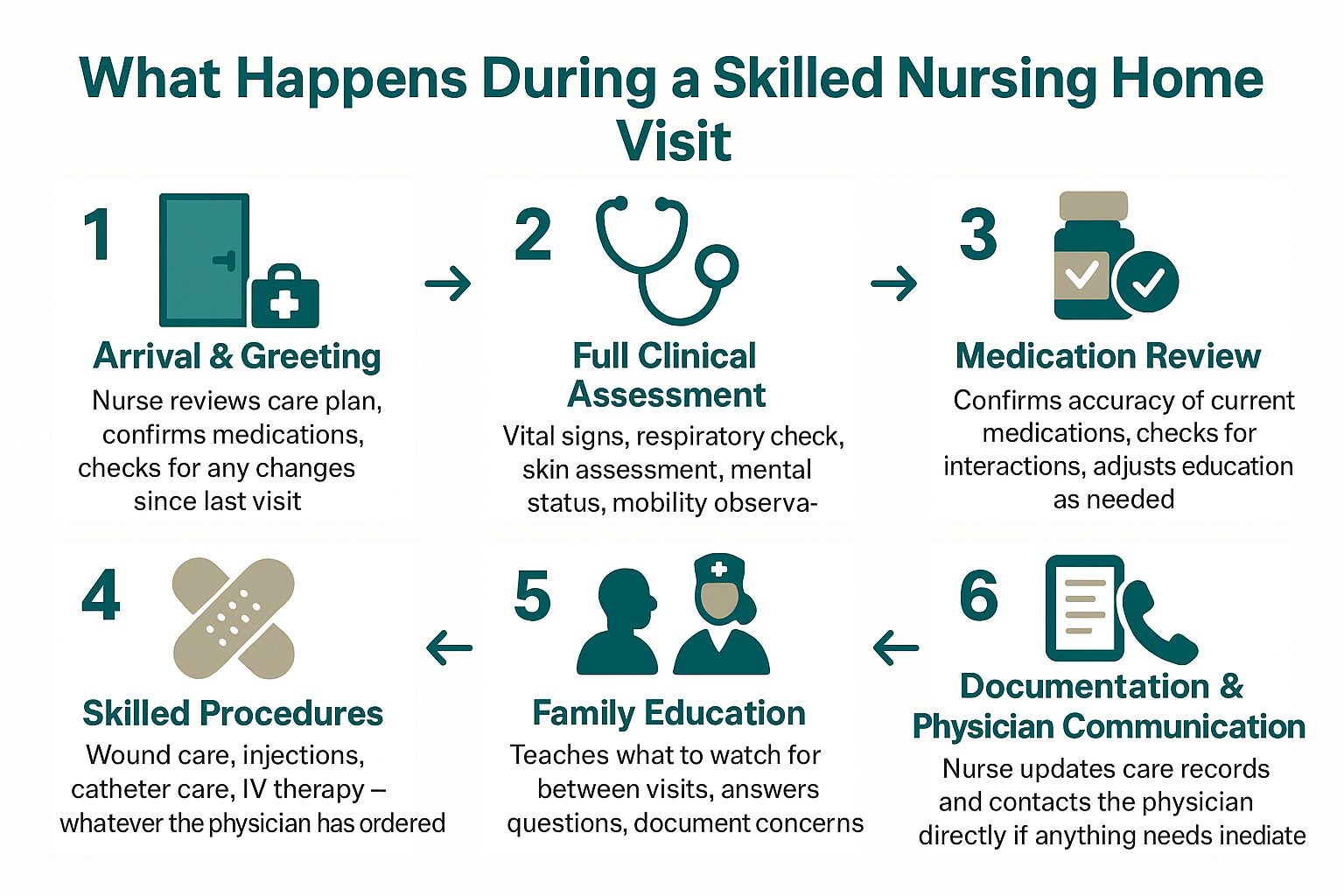
By the end of the first visit, the nurse has:
- Completed a full physical assessment
- Reviewed every medication for accuracy, interactions, and adherence
- Identified safety concerns in the home
- Set goals with the patient and family
- Contacted the physician if anything needs to be addressed immediately
What Skilled Nurses Are Actually Watching For
Follow-up visits — which may happen two to three times per week depending on the care plan — are focused and clinical. The nurse isn't just stopping by. They're tracking specific indicators that tell them whether the patient is improving, plateauing, or heading toward a problem.
For someone recovering from cardiac surgery, that might mean monitoring fluid retention and checking whether ankles are swelling. For a patient with diabetes, it means reviewing blood sugar logs and looking at any wounds on the feet. For someone on a blood thinner after a stroke, it means watching for signs of bleeding or new neurological changes.
This kind of close monitoring is what many Monterey families didn't realize was available at home until they needed it.
Common clinical tasks during a skilled nursing visit include:
- Blood pressure, pulse, respiratory rate, and oxygen saturation monitoring
- Wound assessment and dressing changes — including surgical incisions, pressure injuries, and diabetic ulcers
- Medication reconciliation — confirming the patient is taking the right doses at the right times, and flagging anything that changed at discharge
- IV therapy or injections when ordered by the physician
- Catheter care
- Patient and family education — teaching family members what to watch for between visits
The education piece matters more than most families expect. A skilled nurse will walk a spouse or adult child through how to recognize signs that something is wrong — what shortness of breath looks like in someone with CHF, or when a wound needs to be called in to the physician. That knowledge is what keeps people out of the emergency room at 2 a.m.
A Typical Skilled Nursing Visit: What Happens and When
This breakdown shows the general flow of a skilled nursing home visit — from arrival to documentation — so families know what to expect.
When a Nurse Notices Something the Doctor Hasn't Seen Yet
One thing families consistently underestimate is how much clinical information a home nurse captures that a clinic visit never would.
In a physician's office, a patient is there for 15 to 20 minutes, often in their best condition — dressed, alert, accompanied by a family member who's managing the situation. At home, a nurse sees how that same person actually functions. Do they forget to take their medication until reminded? Do they struggle to get up from the couch? Are they eating?
For patients managing chronic illness in communities like King City or Hollister — where the nearest specialist might be an hour away — this kind of close, repeated observation is often what catches a decline early enough to do something about it.
Skilled nurses are required to communicate changes to the ordering physician. If a patient's weight jumps 5 pounds in 48 hours — a common early warning sign of fluid retention in heart failure patients — the nurse calls the physician that day. That call may result in a medication adjustment that prevents hospitalization. That's not a routine checkup. That's active clinical management.
It's also worth understanding that skilled nursing works best as part of a team. Depending on the care plan, a patient might also be receiving visits from Physical Therapists, Occupational Therapists, Speech Therapists, or Medical Social Workers — all coordinated under the same plan. Staying home as health needs change depends heavily on that kind of coordination working smoothly.
Skilled Nursing vs. Home Health Aide: What's the Difference?
Families often confuse skilled nursing visits with home health aide services. They're not the same thing, and insurance coverage reflects that distinction.
| Skilled Nurse (RN or LVN) | Home Health Aide | |
|---|---|---|
| Training required | Licensed RN or LVN | Certified Home Health Aide (CHHA) |
| What they do | Clinical assessment, wound care, medication management, IV therapy, physician communication | Bathing, dressing, grooming, light household tasks |
| Can administer medications? | Yes | No |
| Medicare coverage | Covered when medically necessary and homebound criteria are met | Covered only when skilled nursing or therapy is also being received |
| Who orders the visits? | Physician order required | Physician order required (as part of the broader home health plan) |
| Typical visit length | 45–90 minutes | 2–4 hours |
Does Medicare Cover Skilled Nursing at Home?
Medicare Part A covers skilled nursing visits at home when three conditions are met: the patient is considered homebound, a physician has ordered the care, and the services are provided by a Medicare-certified home health agency.
'Homebound' doesn't mean bedridden. It means leaving home requires a considerable effort — using a walker, needing assistance, or risking your health by going out. Most patients recovering from surgery or managing serious illness qualify.
When those criteria are met, Medicare covers skilled nursing visits at no cost to the patient — no copay, no deductible for the home health benefit. That's meaningful for families in Monterey County where the cost of care adds up quickly.
Medi-Cal and Veterans benefits also cover home health services, and understanding what happens when Medicare doesn't cover everything is worth reading if your family is working through the financing piece.
One practical note: skilled nursing visits are not the same as private-pay companion care or housekeeping services. Those are separate, not covered by Medicare, and serve a different purpose. If you're trying to figure out when home care is even the right step, starting with what Medicare covers is usually the most useful first question.
Frequently Asked Questions About Skilled Nursing Home Visits
How often does a skilled nurse visit?
It depends on the care plan and what the physician orders. Right after a hospital discharge, visits might happen three to five times per week. As the patient stabilizes, visits typically taper to once or twice a week. The frequency is always based on clinical need, not a set schedule.
Does my parent have to be bedridden to qualify for home nursing?
No. The Medicare definition of 'homebound' is broader than most people think. Someone who can walk short distances but finds it taxing, or who needs help getting in and out of a car, likely qualifies. A physician makes that determination based on the patient's specific condition.
What's the difference between a Registered Nurse and a Licensed Vocational Nurse on a home visit?
Both RNs and LVNs perform skilled nursing visits at home, but their scope of practice differs. Registered Nurses have a broader clinical scope — they conduct the initial assessment, develop the care plan, and handle more complex clinical situations. Licensed Vocational Nurses work under RN supervision and handle many of the ongoing visit tasks like wound care, medication management, and vital sign monitoring. For most families, both represent competent, trained clinical care.
Can the nurse communicate directly with my parent's specialist in San Francisco or Stanford?
Yes. Skilled nurses document every visit and are required to report significant changes to the ordering physician — regardless of where that physician is located. If your parent sees a cardiologist in San Francisco but lives in Monterey, the home nurse coordinates with that physician by phone, fax, or electronic health record. Distance doesn't prevent that communication.
What happens if the nurse finds something serious during a visit?
The nurse contacts the physician immediately and documents the finding. Depending on the situation, this might result in a same-day medication change, an order for lab work, or a recommendation to go to the emergency room. If the situation is life-threatening, the nurse calls 911. Home nurses are trained to triage exactly these moments — it's one of the reasons close monitoring at home can prevent hospitalizations.
Is skilled nursing the same as palliative care or hospice?
No — though they can overlap. Skilled nursing is a medical service focused on recovery, chronic disease management, and post-hospital care. Palliative care adds a layer of symptom management and care planning for serious illness — and doesn't require giving up other treatment. Hospice is specifically for end-of-life care. You can learn more about what palliative care actually means for families if that's the direction your family is considering.
Questions About Home Nursing for a Family Member in Monterey County?
Central Coast VNA & Hospice has been providing skilled nursing care to families across Monterey County, Santa Cruz County, San Benito County, and South Santa Clara County since 1951. If you're trying to sort out whether a loved one qualifies, what a care plan might look like, or what to ask their physician, a care coordinator can walk you through it without any pressure. Call 831-372-6668 or visit ccvna.com to start that conversation.

The Difference Between Needing Help and Needing a Facility
When a parent's health starts to slip, the mind goes straight to the hardest question: do we need to move them somewhere? It's one of the most emotionally loaded decisions a family can face — and in Monterey County, it's a question thousands of families work through every year without a clear roadmap.
But here's what often gets missed: needing help is not the same as needing a facility. A lot of families assume those are the only two options — either you manage everything yourself, or you start looking at skilled nursing facilities in Salinas or memory care units on the Peninsula. There's a wide middle ground that most people never fully explore.
This guide is for families trying to understand what home-based care can actually handle — and where the real line is between that and facility-level care. No sales pitch. Just a clear-eyed look at what the options actually mean.
What 'Needing Help' Actually Looks Like
Most families recognize something is off before they can name it. Dad is slower getting up. Mom missed two doses of her blood pressure medication. A fall happened — or almost happened. These are signals, but they don't automatically mean a facility is the answer.
Home-based support exists precisely for this stage. Skilled nursing visits, physical therapy, medication management, wound care after a surgery — these are all services that can come to your loved one's home in Monterey, Salinas, Hollister, or King City without uprooting their life.
The kinds of situations that respond well to home-based care include:
- Recovery from a hospital stay or surgery
- Managing a chronic illness like heart failure, COPD, or diabetes
- Wound care that requires a Registered Nurse's assessment
- Physical therapy after a hip or knee replacement
- Medication reviews and adjustments supervised by a clinician
- Early or moderate cognitive changes where the person is still safe at home
None of these automatically require a facility. And for many families, understanding what home care can realistically provide changes the entire conversation.
The goal of home-based skilled care isn't to avoid hard decisions indefinitely — it's to make sure families aren't making those hard decisions prematurely, before they've tried what's actually available to them.

Where the Real Line Is: When a Facility Becomes Necessary
Home-based care has real limits, and it's important to name them honestly.
A facility becomes the right answer when the level of supervision or medical complexity exceeds what can be safely managed — even with daily visits from nurses and therapists. 24-hour supervision, certain types of wound care requiring constant monitoring, or situations where a person can no longer be left alone safely for any stretch of time are examples where the home setting may no longer be appropriate.
Some specific indicators that point toward facility-level care:
- The person is a fall risk who cannot be left unsupervised at any point during the day or night
- They require ventilator support or IV therapy that can't be managed intermittently
- Behavioral symptoms of dementia — aggression, wandering, or severe disorientation — have become unsafe for everyone in the home
- The primary family support in Salinas, Pacific Grove, or wherever they live has reached a point of physical or emotional exhaustion that creates a safety risk
- Round-the-clock hands-on assistance with eating, bathing, and repositioning is required every few hours, not just once or twice a day
These are specific, clinical thresholds. And reaching one of them doesn't mean failure — it means the situation has changed, and the right support has to change with it.
For families navigating serious illness who haven't reached that threshold, palliative care at home often provides the symptom management and care coordination that keeps people safely in place far longer than families expect.
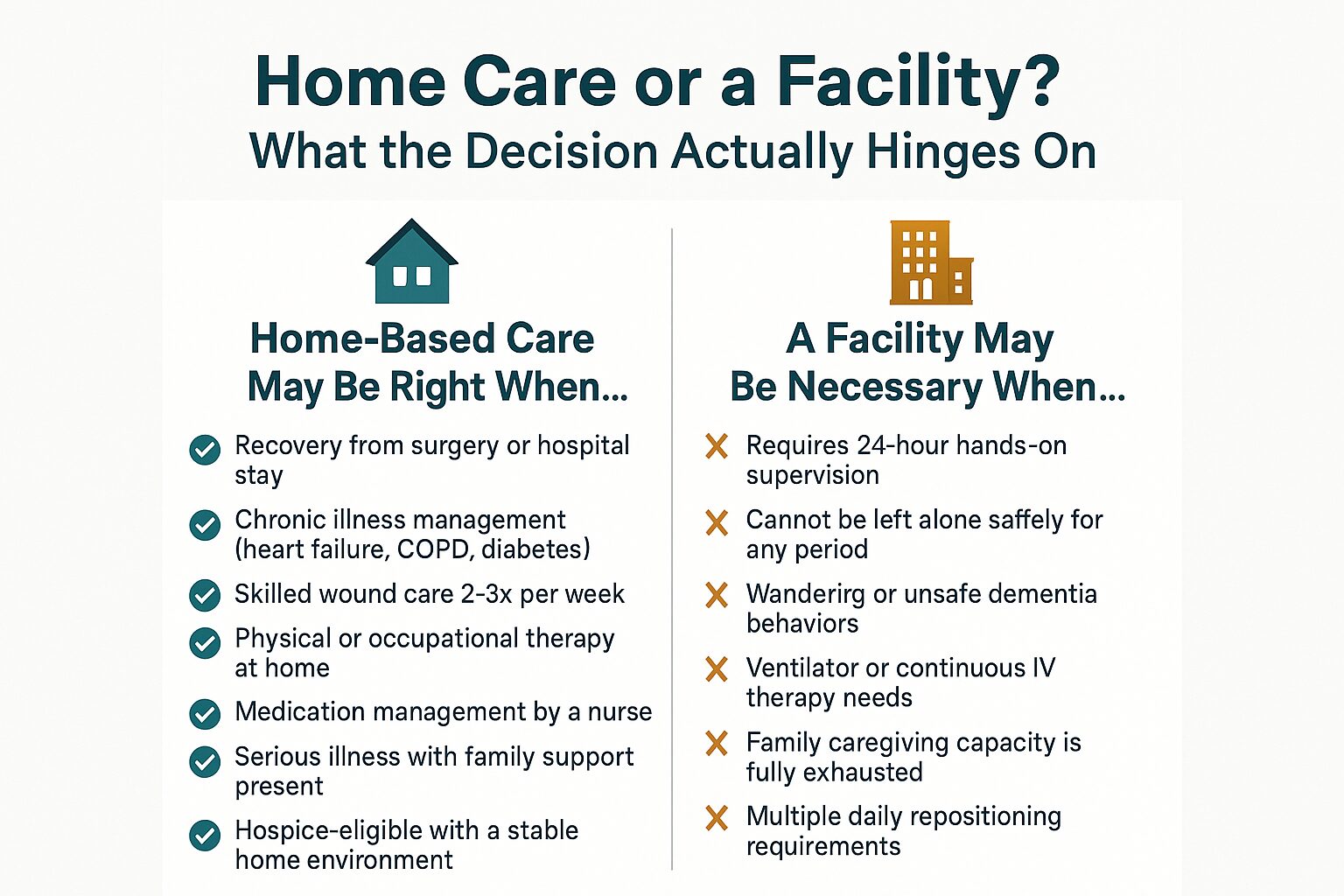
Home Care vs. Facility Care: How the Decision Actually Works
This breakdown shows the key factors that separate home-based care from facility-level care — and what the decision hinges on for most Monterey County families.
What Medicare Actually Covers at Home — and What It Doesn't
One reason families jump to facility thinking is cost uncertainty. They don't know what Medicare covers at home, so they assume a facility is the only structured option.
Medicare covers skilled home health services when a physician certifies that the patient is homebound and needs skilled nursing, physical therapy, occupational therapy, or speech therapy. That coverage is meaningful — it includes Registered Nurse visits, Licensed Vocational Nurse visits, therapy sessions, and Medical Social Worker support, all without a copay under traditional Medicare Part A and B.
What Medicare does not cover at home:
- Custodial care — help with bathing, dressing, and meals — unless it accompanies a skilled service
- 24-hour home supervision
- Long-term personal care without a skilled medical need
Medi-Cal can fill some of those gaps for qualifying patients in Monterey County. And for families facing end-of-life situations, the Medicare Hospice Benefit covers a wide range of services — nursing, aide support, medications related to the terminal diagnosis, chaplain visits, and bereavement support — with no cost-sharing for Medicare beneficiaries.
Veterans receiving care through VA benefits may have additional options worth exploring through a Medical Social Worker.
For a closer look at how coverage works, this breakdown of Medicare home health coverage walks through what's included and how to know if a patient qualifies.
Home Care vs. Facility Care: A Side-by-Side Look
This table gives families a concrete comparison of what each setting typically provides and what it costs in the Monterey County area.
| Factor | Home-Based Skilled Care | Skilled Nursing Facility |
|---|---|---|
| Setting | Patient's own home | Residential facility |
| Medicare coverage | Covered when homebound + skilled need certified | Covered for short-term rehab stays (up to 100 days) |
| Typical out-of-pocket cost (Monterey County) | $0 copay for Medicare-covered skilled visits | $194.50/day after day 20 (2024 Medicare rate) |
| Who provides care | RNs, LVNs, PTs, OTs, Social Workers, Aides on scheduled visits | On-site nursing staff 24 hours/day |
| Level of supervision | Intermittent — visits, not constant presence | Continuous staff availability |
| Best suited for | Recovery, chronic illness management, serious illness with family support | High-acuity needs, post-acute rehab requiring 24-hour oversight |
| Patient autonomy | Full control over environment, routine, diet | Structured facility schedule and environment |
| Hospice eligible | Yes — hospice is primarily delivered at home | Yes — hospice can be provided in facilities too |
The Conversation Families Avoid — and Why It Matters
Most families put off this conversation until something forces it — a hospitalization, a bad fall, or a crisis that lands everyone in an ER waiting room at midnight. By then, decisions get made under pressure instead of with clarity.
Having the conversation earlier — when a parent is still relatively stable — is one of the most practical things a family can do. It's not morbid. It's the opposite: it protects the person's ability to stay in their own home longer, because you've identified what support would make that possible before a crisis strips away those options.
For families in Pacific Grove, Carmel, Hollister, or anywhere across Monterey County, knowing when to start thinking about home care is the kind of guidance that changes outcomes — not because it speeds anything up, but because it gives families more real choices.
And for those dealing with a serious illness diagnosis, palliative care is often the missing piece. It doesn't replace treatment, and it doesn't mean giving up. It means a team of nurses, therapists, social workers, and chaplains is actively managing symptoms and supporting the family while the patient continues receiving care.
Frequently Asked Questions About Home Care vs. Facility Care
Can someone with dementia stay at home with skilled care support?
Often, yes — for a significant portion of the illness. The determining factor isn't the diagnosis itself but the level of supervision required and the safety of the home environment. Early to moderate dementia, where the person is not wandering or posing a physical danger, can frequently be managed at home with a combination of family involvement, skilled nursing visits, and home health aide support. When behavioral symptoms become unpredictable or dangerous, that's when the balance shifts.
My mother just got out of the hospital. Does she automatically qualify for home health?
A hospital stay doesn't automatically qualify someone, but it's one of the most common pathways. Medicare requires that a physician certify the patient as homebound (meaning leaving home requires considerable effort) and that there is a skilled need — nursing, therapy, or both. Discharge planners at hospitals in Salinas or Monterey can initiate the referral before the patient even leaves.
Is hospice only for the last few days of life?
No — and this is one of the most damaging misconceptions families carry. Hospice is available when a physician certifies that a patient has a life-limiting illness with a prognosis of six months or less if the disease follows its expected course. Many patients receive hospice care for weeks or months, not just days. Families who access hospice earlier consistently report better pain control and more time to focus on what matters. You can read more in this guide to hospice care for families.
What if we can't afford a facility but aren't sure home care is enough?
Talk to a Medical Social Worker before making any decisions. They can assess the actual clinical picture, map out what Medicare or Medi-Cal covers, and identify realistic options — including whether the level of need actually calls for a facility at all. In many cases, families who assume they need a facility find that structured home-based care with the right clinical team covers what's needed.
What happens to the family after a loved one passes — does support end?
Bereavement support continues after a patient's death. Families who received hospice care have access to grief counseling and ongoing emotional support through bereavement specialists — typically for at least 13 months following the loss. Bereavement support services are also available to community members in Monterey County who didn't receive hospice care through VNA.
Not Sure Which Direction Makes Sense for Your Family?
Central Coast VNA & Hospice has been walking alongside families in Monterey County, Salinas, Hollister, and the surrounding Central Coast since 1951 — including families facing exactly the kind of decision this article is about. A care coordinator can help you think through what your loved one's situation actually calls for, without pressure and without guesswork. Call 831-372-6668 or visit ccvna.com to start that conversation.

What Families in Monterey Wish They'd Known Sooner About Home Care
Most families in Monterey County don't think about home care until a parent falls, a hospital stay ends abruptly, or a diagnosis lands that nobody was ready for. Then the questions come fast — and the answers feel impossibly hard to find.
What actually surprises people, once they're on the other side of that moment, is how much was available to them all along. Skilled nursing at home. Physical therapy in the living room. Help managing a chronic illness without driving to Salinas or Pacific Grove three times a week.
This article is built around the things families consistently say they wish they'd understood earlier — not about any one service, but about how home-based care actually works, what it costs, and when to start the conversation.
The Part About Medicare Nobody Explains Clearly
When a parent comes home from Community Hospital of the Monterey Peninsula after a surgery or a health event, the discharge process moves fast. A nurse hands over paperwork, someone mentions "home health," and families nod along — often without fully understanding what they just agreed to or what they're entitled to.
Medicare covers more than most families realize. If your parent is homebound and a physician certifies that skilled care is needed, Medicare Part A will pay for:
- Skilled nursing visits from a Registered Nurse or Licensed Vocational Nurse
- Physical therapy, occupational therapy, and speech therapy at home
- Medical social worker visits
- Some medical equipment and supplies
There is no copay for Medicare-covered home health services, and there's no requirement that your parent have a prior hospital stay to qualify. That surprises almost everyone.
What Medicare doesn't cover is around-the-clock supervision or personal care that isn't tied to a medical need. Understanding that line — between skilled care and custodial care — saves families from a lot of confusion later. For a deeper look at what happens when coverage has gaps, Can I Still Get Home Care If Medicare Doesn't Cover Everything? is worth reading before you need it.
Medi-Cal and Veterans benefits also cover home health services for qualifying patients, and those programs serve a significant portion of families across Monterey County, Salinas, and Hollister.

When to Ask for Help — and Why Families Usually Ask Too Late
There's a pattern that plays out in families across Monterey County, from Carmel Valley to King City. A parent starts declining slowly — missing medications, losing weight, struggling with balance — and family members rationalize each change as a one-off. By the time someone calls for help, the situation is harder to manage than it needed to be.
The signs that warrant a conversation with a physician or a home health organization aren't dramatic. They're quiet.
- Repeated falls or near-falls in the past 90 days
- A new diagnosis that requires ongoing monitoring (heart failure, COPD, diabetes)
- A surgery recovery happening at home without clinical follow-up
- Wounds that aren't healing or are getting worse
- Medications that are confusing or being taken inconsistently
- Noticeable changes in strength, balance, or the ability to speak clearly
Any one of those is a legitimate reason to ask a physician whether home health services are appropriate. The bar isn't "my parent can't function at all." The bar is: is there a clinical need that could be safely addressed at home?
For families trying to figure out where that line actually falls, When Is It Time to Think About Getting Help at Home? gives a more detailed breakdown of the signals worth taking seriously.
Home Health vs. Palliative Care vs. Hospice — What's the Difference?
Families often use these terms interchangeably, but they describe three different things. Here's a plain-language comparison of what each one involves.
| Type of Care | Who It's For | Key Services | Medicare Coverage |
|---|---|---|---|
| Home Health | Patients recovering from illness, surgery, or managing a chronic condition | Skilled nursing, physical/occupational/speech therapy, wound care, medication management | Yes — if homebound and physician-ordered |
| Palliative Care | Patients with serious illness at any stage, including those still receiving treatment | Symptom management, care planning, emotional support, coordination with treating physicians | Partially — varies by service and payer |
| Hospice | Patients with a terminal diagnosis and a life expectancy of 6 months or less | Pain management, interdisciplinary team support, spiritual care, family guidance, bereavement | Yes — Medicare Hospice Benefit covers nearly all costs |
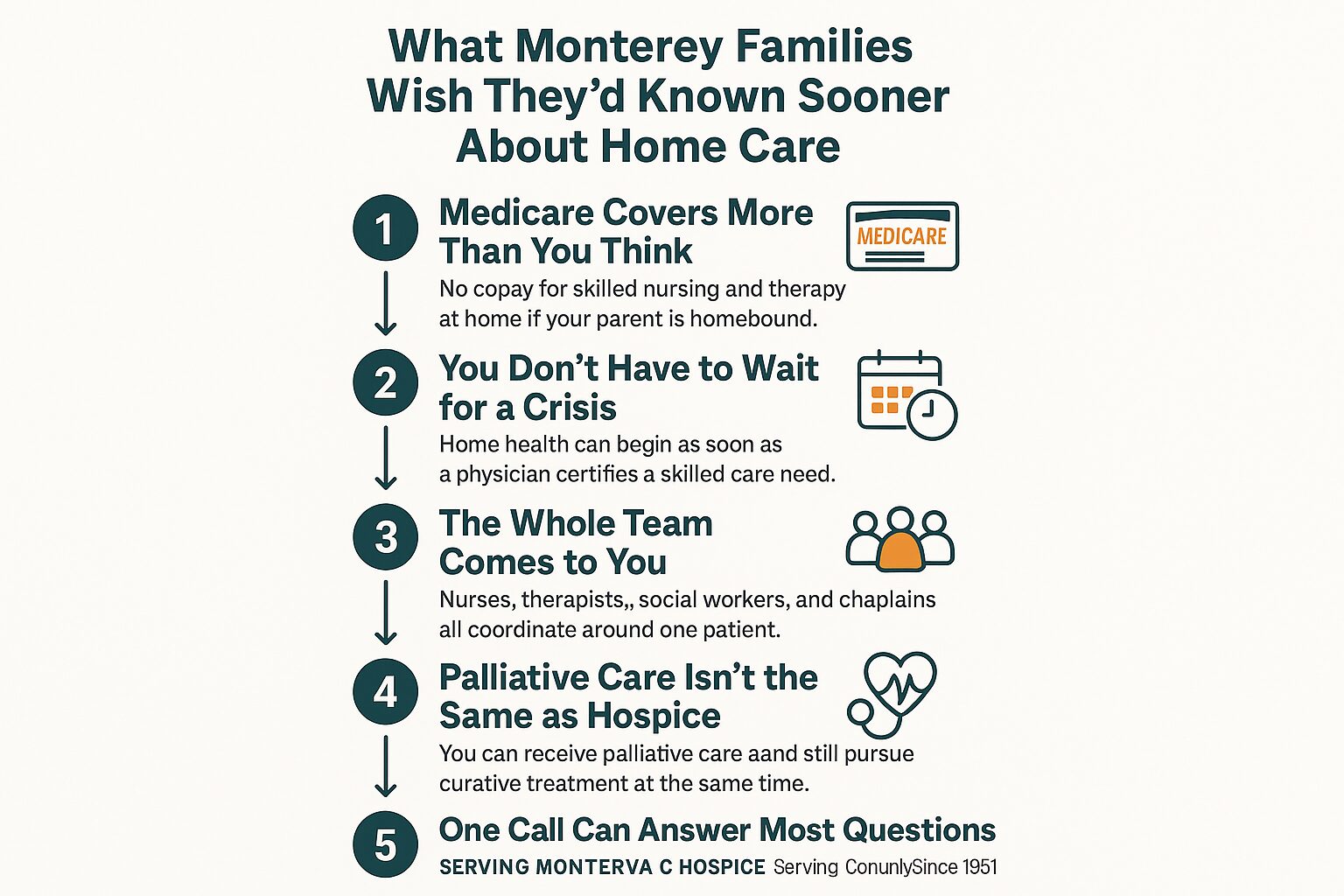
The 5 Things Monterey Families Wish They'd Known Sooner
These are the five points that come up most consistently when families reflect on what they would have done differently.
What Palliative Care Actually Means for a Family in the Middle of It
"Palliative" is one of those words that stops people cold. Families often assume it means their loved one is being given up on — that it's a step toward hospice, not away from suffering.
That's not what it is.
Palliative care is symptom management and support for people living with serious illness, and it can happen alongside any other treatment a physician is providing. Someone in Salinas going through chemotherapy can receive palliative care at the same time. Someone in Pacific Grove managing advanced heart disease can have a palliative care team helping with pain, breathlessness, and care planning — while still seeing their cardiologist.
The team that delivers palliative care typically includes nurses, Medical Social Workers, and sometimes Chaplains or other clinicians depending on what the patient needs. Visits happen at home. The focus is on quality of life and making sure the patient — and the family — understands what's happening and what choices are available.
For a much more detailed explanation of what this looks like in practice on the Central Coast, Palliative Care Meaning: A 2026 Guide to Family Support is a good place to start.
One thing families consistently say: they wish they'd asked about palliative care months earlier. It doesn't foreclose any options. It adds support.
Hospice at Home — What It Looks Like in Real Life
People picture hospice as a facility — a quiet building somewhere outside of town. In Monterey County, most hospice care happens at home. The patient stays in their own bedroom, in a house they know, surrounded by people who matter to them.
The hospice team visits regularly. That team isn't just a nurse. It includes:
- Registered Nurses managing pain and symptoms
- Hospice Aides helping with personal care and comfort
- Medical Social Workers supporting the patient and family emotionally and practically
- Chaplains available for spiritual support — regardless of religious background
- Volunteers who provide companionship and relief for family members
- Bereavement Specialists who continue working with the family after the patient passes
The Medicare Hospice Benefit covers nearly everything — medications related to the terminal diagnosis, equipment like hospital beds or wheelchairs, and all team visits. For families who have spent months managing costly care, that often comes as a genuine relief.
And the conversation about hospice doesn't have to be a final door closing. For many families across the Central Coast, it's the moment things get quieter — and more manageable. The Heart of Hospice: A Guide for Families goes into much more depth on what that transition actually looks like day to day.
If your family is earlier in that conversation and still weighing options, What Is Aging in Place? A Guide for Central Coast Families addresses how home-based care at every stage fits into the broader goal of staying home.
Frequently Asked Questions About Home Care in Monterey County
Does my parent have to be completely homebound to qualify for Medicare home health?
Not completely housebound — but leaving home has to require considerable effort. Someone who can only go out for medical appointments, or who needs a wheelchair or significant assistance to leave, generally qualifies. A physician makes that determination based on your parent's specific situation.
What's the difference between home health and having a home health aide come in?
Home health under Medicare refers to skilled clinical services — nursing, therapy, wound care — provided by licensed clinicians. A home health aide visit can be part of a Medicare-covered home health plan, but only if it's paired with a skilled care need. Personal care alone — help with bathing, dressing, cooking — is generally not covered by Medicare.
Can someone receive palliative care and still get curative treatment at the same time?
Yes. That's one of the most important things to understand about palliative care. It's not a replacement for treatment — it runs alongside it. A patient can continue working with their oncologist or cardiologist while a palliative care team manages symptoms and supports the whole family.
How does grief support work after a loved one passes?
Bereavement support through a hospice organization typically continues for at least 13 months after a patient's death. That includes check-in calls, counseling resources, and support groups depending on what the family needs. This support is part of the hospice benefit and available to family members — not just the patient. Bereavement Counseling: A Guide to Grief Support covers what to expect during that period.
We live in Hollister — does home care reach us?
Yes. Home-based services in San Benito County, including Hollister, are covered. Monterey County is the largest service area, but families in Hollister and surrounding communities in San Benito County have access to the same skilled nursing, therapy, and hospice services.
How do I even start this conversation with my parent?
That's usually the hardest part. Most families find it easier to frame it around a specific event — a recent fall, a new diagnosis, a medication that's gotten complicated — rather than a general conversation about aging. Focusing on what's already happening, rather than what might happen, tends to feel less threatening to the parent. A Medical Social Worker can also help families navigate that conversation directly.
Ready to Get Some Clarity?
If anything in this article raised a question you haven't been able to answer, a care coordinator at Central Coast VNA & Hospice can talk through your family's specific situation — no commitment required, just information. VNA has been serving families across Monterey County, Salinas, Hollister, and the surrounding Central Coast since 1951, and that experience shows up in every conversation. Call 831-372-6668 or visit ccvna.com to learn more.

Staying Home as You Age — What Actually Makes It Possible?
Most older adults on the Monterey Peninsula will tell you the same thing when asked where they want to spend their later years: home. Not a facility. Not somewhere unfamiliar. The house they know, the neighborhood they've walked for decades, the kitchen where everything is exactly where they left it.
But wanting to stay home and actually being able to stay home are two different things. Families across Monterey County — from Pacific Grove to Salinas to King City — are figuring out that gap right now, often in the middle of a health crisis that didn't leave much time to plan.
This article focuses on two things that matter most: what actually breaks down when aging at home gets hard, and what kinds of support can close those gaps before a crisis forces a different decision.
The Honest Reasons Aging at Home Gets Hard
Most families don't run into trouble because their parent or loved one is simply "getting older." They run into trouble when one specific thing changes — a fall, a new diagnosis, a medication that's harder to manage, a surgery with a recovery that takes longer than expected.
In Monterey County, where many older adults live in homes built in the 1950s and 60s — stairs, narrow bathrooms, no grab bars — the physical environment is often the first problem. A house that worked fine at 65 can become genuinely hazardous by 80.
But the medical side is usually what families underestimate. Conditions like congestive heart failure, COPD, diabetes, and post-stroke recovery require ongoing clinical monitoring. Missing a medication dose or missing an early warning sign isn't a minor inconvenience — it's how people end up in the emergency room at Salinas Valley Health or Community Hospital of the Monterey Peninsula.
The most common breaking points look like this:
- A hospitalization that leaves someone weaker than before, with new medications and new restrictions
- A chronic condition that was manageable until it wasn't
- A family member who was doing most of the daily support and is now overwhelmed or unavailable
- Cognitive changes that make self-care unreliable
If any of these sound familiar, you're already in the window where knowing when to get help at home becomes a real question — not a distant one.

What Skilled Home Health Actually Does (and What It Doesn't)
There's a lot of confusion about what "home health" means. Many families assume it means someone comes to help with bathing and groceries. That's not skilled home health — that's personal care, and it's a separate category entirely.
Skilled home health is medical care delivered in the home by licensed clinicians. That includes Registered Nurses, Licensed Vocational Nurses, Physical Therapists, Occupational Therapists, Speech Therapists, and Medical Social Workers. These are the same credentials you'd see in a hospital or outpatient clinic — just delivered where the patient actually lives.
In practice, skilled home health covers things like:
- Wound care after surgery or from a chronic condition like diabetes
- Medication management — making sure the right drugs are being taken at the right doses, watching for interactions
- Post-surgical recovery — physical and occupational therapy in the home, where the actual environment can be assessed
- Chronic disease management for conditions like heart failure, COPD, and diabetes
- Speech therapy after a stroke or neurological event
One thing that surprises many families: Medicare covers skilled home health when a physician certifies that the patient is homebound and needs skilled care. You can read more about exactly how that works for physical therapy specifically at does Medicare cover physical therapy at home.
What skilled home health does not cover is ongoing personal assistance — help getting dressed every morning, meal prep, transportation. That requires a different type of arrangement, usually paid privately or through certain Medi-Cal programs. Understanding that line early saves families a lot of frustration.
For families in communities like Hollister or King City, where driving to outpatient appointments is a real burden, receiving therapy and nursing at home removes a barrier that would otherwise mean skipping care entirely.
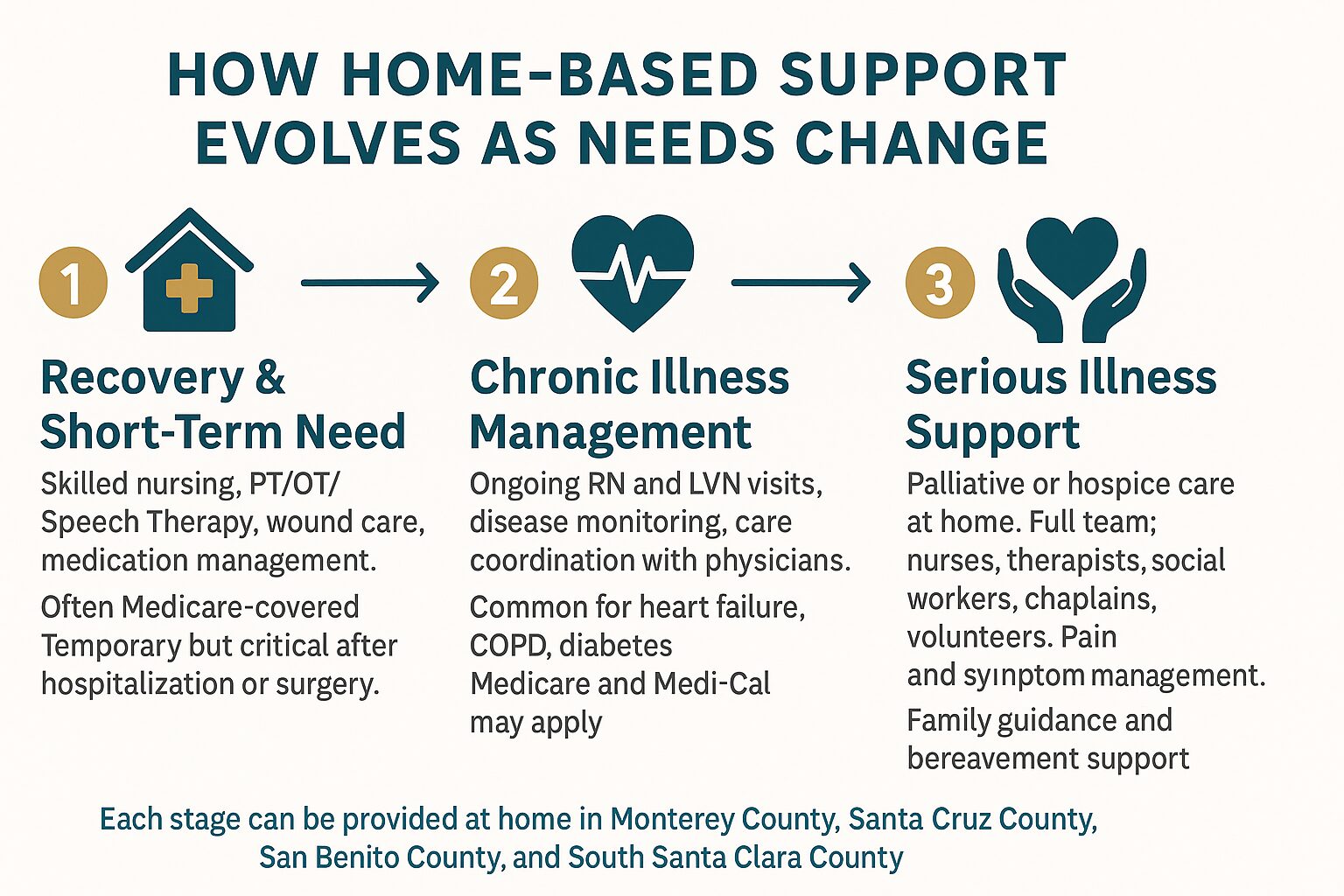
How Home-Based Support Changes Over Time
As health needs shift, the type of support that makes staying home possible shifts too. This breakdown shows how care typically evolves across different stages.
When Palliative or Hospice Care Enters the Picture
At some point, the goal of care shifts. It's not about recovering from something — it's about living as well as possible with something that isn't going away.
That's where palliative care becomes relevant. Most people have heard the term but aren't sure what it means in practice. It doesn't mean giving up treatment. It means adding a layer of support — symptom management, care planning, emotional support — alongside whatever other care is already happening. A Nurse Practitioner or Registered Nurse might visit the home to manage pain. A Medical Social Worker might help the family process what's ahead. A Chaplain might sit with the patient through something a physician doesn't have time for.
You can find a thorough explanation of what this actually looks like for families at palliative care meaning: a guide for families.
Hospice care is a separate level of care for people whose illness is terminal and who have chosen to focus on comfort rather than curative treatment. It brings an interdisciplinary team — nurses, hospice aides, chaplains, volunteers, social workers, and bereavement specialists — directly into the home. It is covered by Medicare and most Medi-Cal plans at no cost to the patient.
What hospice makes possible is something that matters deeply to most families: a loved one spending their final weeks or months at home, surrounded by familiar things, without the burden of constant hospital visits. The heart of hospice is a good starting point if your family is trying to understand what that actually looks like day to day.
For families in Monterey County facing these decisions, the question isn't usually whether to pursue palliative or hospice care — it's when to ask. Asking earlier, before a crisis, leaves families with far more choices.
Skilled Home Health vs. Palliative Care vs. Hospice: A Quick Comparison
These three types of home-based care often get confused with each other. Here's how they differ in purpose, timing, and coverage.
| Type of Care | Who It's For | Medicare Coverage |
|---|---|---|
| Skilled Home Health | People recovering from illness, surgery, or managing a chronic condition who need clinical care at home | Covered when physician certifies homebound status and skilled need |
| Palliative Care | People with serious illness at any stage who need symptom management and support alongside other treatment | Partially covered; depends on services and plan — ask your care coordinator |
| Hospice Care | People with a terminal diagnosis choosing comfort-focused care over curative treatment | Fully covered under Medicare Hospice Benefit; also covered by most Medi-Cal plans |
The Practical Side: Safety, Family Roles, and What Families Often Miss
Even with excellent medical support in place, staying home requires some honest planning around the physical environment and family capacity.
In Monterey County, where a significant portion of the housing stock predates modern accessibility standards, a home safety assessment is often the most practical first step. Occupational Therapists who provide home health can evaluate a living space and recommend specific changes — not just grab bars, but lighting, furniture placement, and how to set up a bed or bathroom to reduce fall risk.
Falls are the leading cause of hospitalization for older adults in California, and many happen in the first few weeks after someone comes home from a hospital stay. That window — when someone is weaker than usual, on new medications, in familiar surroundings that suddenly feel less manageable — is exactly when skilled nursing care in Monterey can make the difference between a safe recovery and a return trip to the ER.
Family members also need to be honest about what they can sustain. Adult children in their 50s and 60s who are managing their own work schedules, health, and households are often doing more than they can carry long-term. A Medical Social Worker can help families map out what realistic support looks like — and where gaps exist — without judgment.
A few things families consistently underestimate:
- Medication complexity — managing 8 to 12 prescriptions at home is not straightforward, and errors are common
- Nighttime safety — most falls happen at night, when no one is watching
- Caregiver fatigue — family members burning out quietly, months before they'll admit it
- The gap after discharge — hospitals discharge patients quickly; recovery happens at home, often with less support than families expect
Frequently Asked Questions About Aging at Home in Monterey County
How do we know if my parent actually qualifies for Medicare-covered home health?
A physician needs to certify two things: that your parent is homebound (meaning leaving the home requires considerable effort) and that they need a skilled service — nursing, physical therapy, occupational therapy, or speech therapy. If both conditions are met, Medicare Part A or Part B typically covers the cost. A care coordinator can help you determine eligibility based on your parent's specific situation.
What's the difference between a home health aide and a Registered Nurse visiting at home?
A home health aide helps with personal care — bathing, dressing, light tasks. A Registered Nurse provides clinical care: wound assessment, medication management, disease monitoring, and coordination with physicians. Both can visit the home, but they serve entirely different functions. Medicare covers skilled nursing visits; it does not cover personal aide services.
Can my parent receive palliative care and still continue cancer treatment or other curative care?
Yes. This is one of the most common misconceptions about palliative care. It is not an alternative to treatment — it runs alongside it. A patient can be receiving chemotherapy or dialysis and still have a palliative care team supporting symptom management and care planning at home.
How far in advance should families start thinking about hospice?
Most families say they waited too long. Hospice care can begin when a physician estimates a prognosis of six months or less if the illness follows its expected course. Calling earlier — even to ask questions — gives families more time to plan and more time to benefit from the support. There's no commitment required from an initial conversation.
Does VNA serve areas outside Monterey, like Hollister or King City?
Yes. Central Coast VNA & Hospice serves all of Monterey County — including King City, Salinas, and the Monterey Peninsula — as well as San Benito County (including Hollister), and parts of Santa Cruz County and South Santa Clara County. If you're unsure whether your address falls within the service area, calling 831-372-6668 is the quickest way to find out.
Have Questions About What Support Is Available?
Families across Monterey County — in Salinas, Carmel, Pacific Grove, King City, and Hollister — have been calling Central Coast VNA & Hospice with exactly the questions this article covers for more than 70 years. If you're trying to figure out what kind of help your loved one qualifies for, or just want to talk through what the options look like, a care coordinator is available to help without any pressure. Call 831-372-6668 or visit ccvna.com to start the conversation.

When Is It Time to Think About Getting Help at Home?
Most families don't plan for this moment. One day, a parent is managing fine. The next, you're noticing the dishes piling up, a fall that 'wasn't a big deal,' or a medication schedule that's gotten confusing. If you're a family member in Monterey County asking yourself whether it's time to get some help — you're already asking the right question.
The challenge is that there's no single clear line. Home health isn't just for people at the very end of life. It's also for someone recovering from a hip replacement at Community Hospital of the Monterey Peninsula, managing heart failure in Salinas, or dealing with a wound that isn't healing the way it should.
This guide walks through the real signs that home health support might be needed, what kinds of help are available, and how families across Monterey County — from Pacific Grove to King City — have found their way through this decision.
The Signs Families Usually Spot First
Most families don't recognize the need for home health all at once. It shows up in small things that start adding up.
Some of the clearest early signs include:
- A recent fall, even if it seemed minor at the time
- Medications being skipped, doubled, or taken at the wrong time
- A chronic condition like diabetes or COPD that's gotten harder to manage
- Weight loss that no one can explain
- Wounds, surgical incisions, or skin breakdown that aren't healing
- Confusion or memory changes that are new or getting worse
- Difficulty walking, bathing, or getting in and out of bed safely
- Missed doctor's appointments due to transportation or fatigue
Any one of these can be a signal. More than two or three together usually means it's time to have a real conversation.
For families in Monterey County, geography adds another layer. If your parent lives in Carmel Valley or out near Greenfield, getting to appointments is genuinely hard. Home-based care removes that barrier entirely — a clinician comes to them.

What Home Health Actually Covers
A lot of people picture home health as someone stopping by to help with chores. That's not what skilled home health is. It's clinical care — delivered at home by licensed professionals.
Depending on what a patient needs, a home health team can include:
- Registered Nurses (RNs) and Licensed Vocational Nurses (LVNs) who manage wound care, IV medications, post-surgical recovery, and chronic disease monitoring
- Physical Therapists who work on strength, balance, and mobility — especially after a fall or surgery
- Occupational Therapists who help patients safely manage daily tasks like bathing, dressing, and getting around the home
- Speech Therapists who address swallowing problems, communication issues, and cognitive function
- Medical Social Workers who connect families with community resources, support systems, and care planning
For patients with a serious illness who aren't ready for hospice, palliative care is another option worth understanding. It focuses on symptom relief and quality of life — and patients don't have to give up other treatments to receive it. The palliative care meaning guide explains this in plain terms.
All of these services can happen at home. In Monterey County, that means a clinician coming to your family's actual house — whether that's a condo in Marina or a farmworker family's home in Soledad.
When a Loved One Is Facing Serious Illness
There's a harder version of this question that some families are sitting with: What do you do when a loved one has been told their illness isn't going to get better?
This is where hospice care becomes relevant — and where many families wish they'd asked questions sooner. Hospice isn't about giving up. It's about choosing comfort and dignity over treatments that may no longer help.
A hospice team typically includes nurses, therapists, social workers, chaplains, volunteers, and other clinicians who work together around the patient and the family. Pain is managed. Emotional and spiritual needs are addressed. And family members get support too — before and after their loved one passes.
If you're trying to understand what this care actually looks like in practice, The Heart of Hospice: A Guide for Families is a good place to start.
One of the most common things families say after choosing hospice earlier is that they wish they hadn't waited. Most patients who receive hospice care in Monterey County are eligible for it weeks or months before families ask.
A Simple Way to Think About the Decision
This visual breaks down the four main situations that typically lead families to explore home health — and what kind of support fits each one.
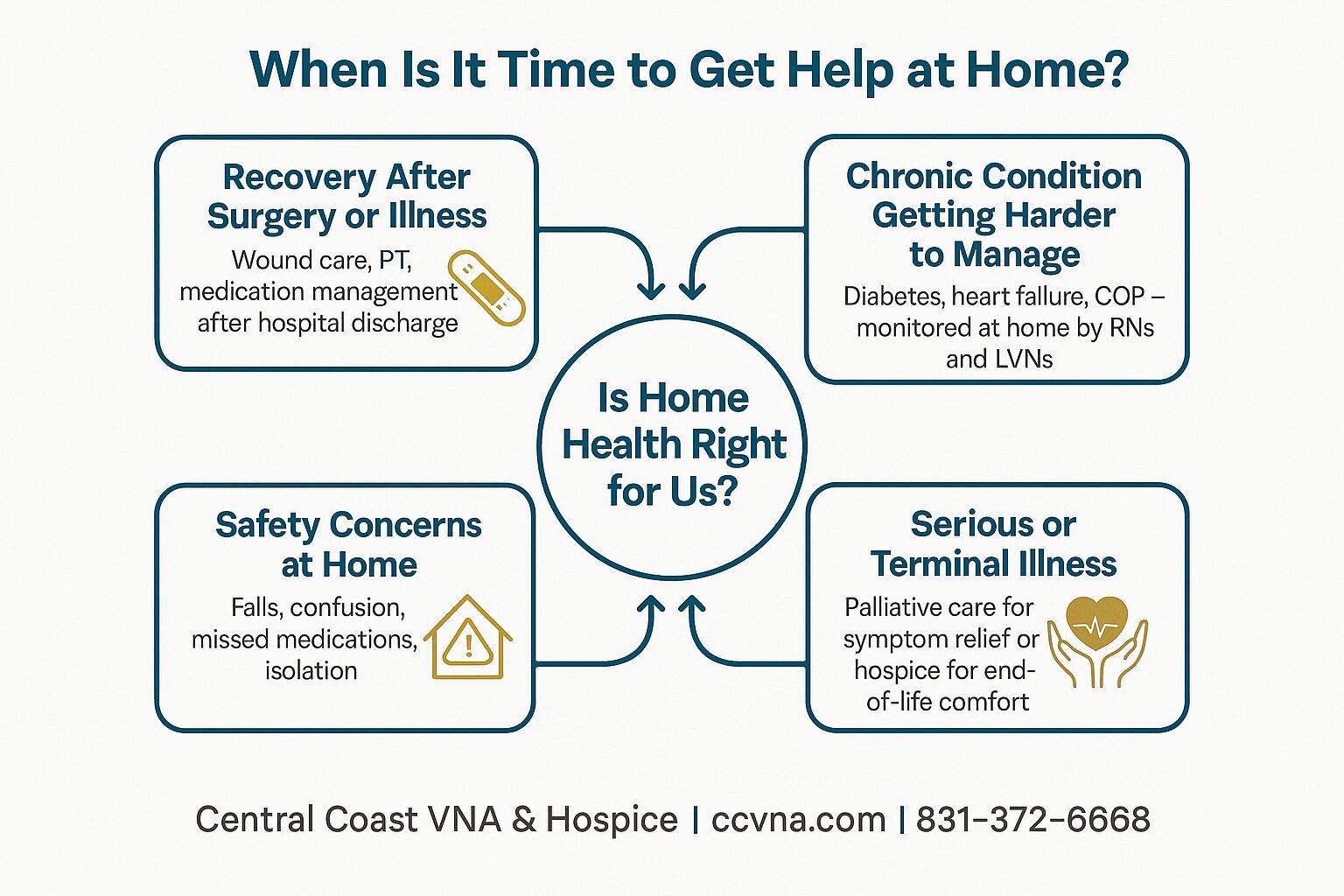
What Medicare and Medi-Cal Actually Pay For
Cost is usually the first question — and the good news is that home health is often more covered than families expect.
Medicare covers skilled home health services when a patient is homebound and a doctor certifies the need. That includes nursing visits, physical therapy, occupational therapy, speech therapy, and medical social work. There's no copay for Medicare-certified home health services when conditions are met.
Medi-Cal covers home health for eligible patients as well. In Monterey County, a significant portion of the population — particularly in Salinas, Greenfield, and King City — qualifies for Medi-Cal, and this is an important coverage option that families sometimes overlook.
Veterans benefits can also cover home health for qualifying veterans. If your family member served, it's worth asking specifically about this.
For a more detailed breakdown of what Medicare covers and what it doesn't, this guide on Medicare and physical therapy at home is useful. And if you're worried about gaps in coverage, this article on what happens when Medicare doesn't cover everything addresses that directly.
The main point: don't assume cost is a barrier before you ask. The answer is often more reassuring than families expect.
Home Health vs. Palliative Care vs. Hospice: What's the Difference?
Families often confuse these three types of care. Here's a straightforward comparison to help clarify when each one applies.
| Type of Care | Who It's For | Does It Require Giving Up Other Treatment? |
|---|---|---|
| Home Health | Anyone recovering from illness/surgery or managing a chronic condition at home | No — this is medical care alongside other treatment |
| Palliative Care | Patients with serious illness who want symptom relief and support | No — patients can continue curative treatment |
| Hospice Care | Patients with a terminal diagnosis choosing comfort over curative treatment | Yes — focus shifts entirely to comfort and quality of life |
The Conversation No One Wants to Have — But Usually Needs To
Bringing up home health with a parent or spouse is hard. Most people resist it at first. It can feel like an admission that something has changed — and no one wants to admit that.
A few things that tend to make the conversation easier:
- Start with a specific concern, not a general one. 'I noticed you were unsteady on the stairs last week' lands better than 'I'm worried about you.'
- Frame it as temporary if it is. Many people need home health for a short stretch after surgery — not forever.
- Ask the doctor to bring it up. Physicians carry authority that family members don't. A recommendation from a doctor at Natividad Medical Center or Salinas Valley Memorial Hospital often lands differently.
- Give the person some control. Letting them be part of the decision — which days, which services — makes acceptance more likely.
If the conversation is about hospice specifically, this guide on aging in place for Central Coast families may help frame the broader picture of care at home in a way that opens the door.
And if grief is already part of the picture — if a family is anticipating a loss or has recently experienced one — bereavement support is available and doesn't require waiting until after a death. Grief support services can start when a family needs them.
How to Know If Home Health Is the Right Fit Right Now
Not every situation requires a full skilled home health team. But there are some clear indicators that it's the right time to make a call and ask.
Home health is likely a good fit if:
- A loved one was just discharged from a hospital or rehab facility and needs follow-up care
- A doctor has recommended home health but the family hasn't acted on it yet
- A chronic condition has caused a recent emergency room visit or hospitalization
- The family lives far from the patient and can't provide daily oversight
- The patient refuses to leave home for appointments — but clearly needs ongoing clinical monitoring
Home health may not be the right fit if someone mainly needs companionship or help with housekeeping. Those are important needs, but they fall under a different category of services.
For families trying to sort through senior home care options in Monterey and surrounding areas, understanding the difference between skilled care and custodial care is an important first step. Skilled care is what Medicare covers. Custodial care — help with bathing, meals, laundry — is a separate conversation.
If you're not sure which one your family needs, a care coordinator can usually help you figure that out in a single phone call.
Frequently Asked Questions About Getting Help at Home
Does my loved one have to be bedridden to qualify for home health?
No. The Medicare definition of 'homebound' doesn't mean completely unable to leave home. It means leaving requires considerable effort — due to illness, injury, or a medical condition. Many people who qualify for home health do leave the house occasionally.
Can my parent stay on home health for as long as they need it?
Home health is typically prescribed in 60-day certification periods, and a doctor must re-certify the need at each renewal. As long as a patient continues to meet the criteria — homebound status and a skilled care need — coverage can continue.
What's the difference between home health and a home health aide?
Skilled home health involves licensed clinicians — RNs, LVNs, physical therapists, and others — providing medical care. A home health aide assists with personal care like bathing and dressing. Medicare covers skilled care; aide services are covered only as part of a broader skilled care plan.
Who decides when it's time for hospice — the family or the doctor?
It's a shared decision. A physician must certify that a patient has a terminal prognosis of six months or less if the illness follows its expected course. But families and patients have a say in when to make that transition — and many wish they'd had the conversation sooner.
What happens to bereavement support after a hospice patient passes away?
Bereavement support doesn't end at the time of death. Hospice programs are required to offer at least 13 months of bereavement follow-up after a patient passes. That can include grief counseling, check-in calls, and emotional support for the whole family.
Ready to Talk Through Your Options?
If you're a family in Monterey County — or in Santa Cruz, San Benito, or South Santa Clara County — and you're trying to figure out whether home health, palliative care, or hospice is the right next step, Central Coast VNA & Hospice has been helping families work through exactly this question since 1951. You can reach a care coordinator at 831-372-6668 or visit ccvna.com to learn more about what's available and whether your loved one may qualify.

Bereavement Couseling: A Guide to Grief Support
The first days and weeks after a loss can feel strangely crowded and empty at the same time. There are phone calls, paperwork, meals left at the door, and moments when the house goes quiet in a way that doesn't feel normal anymore. If you're searching for bereavement couseling, you may not be looking for a formal answer so much as a steady place to land.
Grief rarely moves in a clean line. Some people need company, some need privacy, and some need more structured support than friends and family can give. Bereavement support exists to help you carry the loss, make room for what you're feeling, and figure out what kind of help fits your life right now. If you need gentle ways to put words to what's happening, these grief activities for adults can also be a useful starting point.
Navigating Loss and Finding Your Footing
After someone dies, people often expect themselves to “handle it” because the funeral is over, relatives have gone home, and daily responsibilities are waiting. That pressure can make grief feel lonelier than it already is. It can also make it harder to tell the difference between painful but expected grief and grief that is beginning to interfere with daily life in a deeper way.
Bereavement support gives shape to a time that often feels shapeless. It doesn't ask you to get over the person you lost. It helps you notice what's becoming hard, what support you already have, and what kind of next step might help.
Some families want one private conversation. Others do better in a group, or with support that includes children, teens, faith practices, or cultural mourning traditions. Those differences matter.
Grief support works best when it respects the person, the family, and the relationship that was lost.
If you're in Monterey County or elsewhere on the Central Coast, it may help to know that support can be practical as well as emotional. A good bereavement conversation can include sleep, appetite, family tension, school concerns, anniversaries, and the question many people ask: “Am I doing this wrong?”
Understanding Grief and When to Seek Help
Grief can show up as sadness, anger, numbness, relief, guilt, confusion, forgetfulness, exhaustion, or a strange sense that time has changed shape. You may cry easily. You may not cry at all. You may feel close to other people one day and unable to answer a simple text the next.
That range is one reason grief can be so hard to judge from the inside. People often compare themselves to a sibling, spouse, or friend and assume one person must be grieving “better.” That comparison usually creates more distress, not clarity.

What grief can look like day to day
Some responses are emotional. Some are practical. Some are physical enough that people worry something is wrong with them.
- Emotionally: tearfulness, irritability, anxiety, flatness, or sudden waves of longing
- Mentally: trouble concentrating, indecision, replaying the final days, or feeling detached
- Socially: avoiding calls, withdrawing from gatherings, or feeling unseen around other people
- Functionally: trouble returning to routines, managing bills, making meals, or showing up at work or school
Needing help with these things doesn't mean you're weak. It means loss affects the whole person.
When extra support makes sense
A useful way to think about grief support is that not everyone needs the same level of care. In a population-based survey of bereaved respondents, researchers found that 58.4% were in a low-risk group, 35.2% in a moderate-risk group, and 6.4% in a high-risk group. The same study noted that family and friends were the most-used supports across groups, while mental health professionals were used more often by the high-risk group. The average time since bereavement among respondents was 14.3 months, which is a reminder that grief often lasts well beyond the early period after a death (public health model of bereavement risk and support use).
That matters because one-size-fits-all grief support usually misses the mark. Some people do well with family, friends, rituals, and time. Others need structured counseling. A smaller group needs specialty mental health treatment.
You may benefit from more formal support if:
- Daily life feels stalled: basic tasks, work, parenting, or sleep have become hard to manage
- You feel stuck in one state: numb, panicked, enraged, or unable to re-enter ordinary life
- You're pulling away from everyone: isolation starts to feel safer than being with people
- The loss is affecting judgment: decision-making feels overwhelmed or chaotic
- Substance use or risky coping is appearing: alcohol, medications, or other habits are becoming a way to get through the day
For families who want a clearer picture of what this kind of help can involve, grief counseling for families can be a helpful next read.
Practical rule: Seek help when grief is not only painful, but also making it hard to function, connect, or care for yourself.
What Is Bereavement Couseling?
Bereavement couseling is structured support for people adjusting to life after a death. The point isn't to erase grief or rush you toward acceptance. The point is to help you live with the loss in a way that is more stable, less isolating, and more manageable.
That may sound simple, but in practice it matters a great deal. A good bereavement conversation gives you room to speak openly about the person who died, the circumstances of the death, the parts of grief that embarrass you, and the practical changes that have followed. It can also help when family members are grieving in very different ways.

What counseling is trying to do
Research summarized by Positive Psychology suggests that bereavement therapy can help distressed adults, but that individualized approaches are more effective than routine ones. The goal is a targeted intervention to restore functioning and adaptation, not a fixed number of sympathy visits (individualized grief counseling approaches).
In plain language, that usually means counseling may focus on things like:
| Need | What support may involve |
|---|---|
| Feeling overwhelmed | steady listening, pacing, and grounding |
| Feeling alone in your reactions | normalization and emotional validation |
| Trouble getting through the day | coping tools tied to meals, sleep, routines, and decisions |
| Family strain after the loss | clearer communication and realistic expectations |
| Wanting to stay connected to the person | memory work, rituals, and ways to honor the relationship |
Some people only need a short period of support. Others need more than routine bereavement follow-up and should be referred for specialty mental health treatment. That difference is important. Hospice bereavement services and psychotherapy are related, but they aren't always the same thing.
What counseling is not
Bereavement counseling is not a test you pass by saying the right things. It isn't built around forcing tears, pushing disclosure, or telling you how long grief should last. It also shouldn't ignore serious warning signs in the name of being supportive.
If you want another plain-language resource for understanding grief counseling, that guide can help answer the basic question of what this support is meant to do. Families who are specifically looking at hospice-related grief support can also review hospice bereavement services.
Exploring Different Types of Grief Support
The right support depends on your temperament, your family, the kind of loss, and what feels tolerable right now. Some people need privacy. Others need to hear, out loud, that someone else understands.

Individual support
Individual counseling fits people who want one-on-one space. It can be especially useful when the grief feels complicated, private, or hard to describe in front of others.
You may prefer this route if the death involved family conflict, trauma, estrangement, or strong emotions you're not ready to share in a group. It also helps when you need focused attention on work, sleep, parenting, or a specific anniversary that's approaching.
Group support
A grief group offers something individual counseling can't. It lets you sit with people who are also living through absence. That shared experience often lowers shame and self-doubt.
Group support tends to work well when isolation is becoming part of the problem. It can also help when friends are kind but uncomfortable, or when you're tired of protecting other people from your grief.
Hearing another person describe a feeling you thought was only yours can bring real relief.
If you're looking locally, grief support groups near me may help you think through what kind of group setting feels right.
Family sessions
A death changes the whole family system. One person becomes highly verbal, another shuts down, another takes over logistics, and another becomes angry at small things. None of that is unusual, but it can create tension quickly.
Family counseling can help when grief is colliding with misunderstandings. It gives people room to talk about roles, expectations, memorial traditions, children's questions, and what support at home looks like.
Support for children and teens
Children and teenagers don't grieve like adults. Some return to play quickly. Some ask direct questions. Some show grief through behavior, school problems, physical complaints, or abrupt shifts in mood. Teens may want support but reject anything that feels forced or too adult.
SAMHSA's guidance is useful here because it highlights child-specific resources, peer support, family and community support, faith practices, and culturally grounded rituals. That's an important reminder that talk therapy is only one valid path (coping with bereavement and grief through varied supports).
A simple comparison can help:
| Type of support | Often a good fit for |
|---|---|
| Individual counseling | private processing, complicated feelings, focused coping |
| Group support | loneliness, wanting shared experience, peer connection |
| Family sessions | conflict, different grieving styles, communication problems |
| Child or teen support | developmental needs, school concerns, age-appropriate expression |
| Cultural or faith-based support | mourning practices, identity, family traditions |
Culture matters here too. Mourning is shaped by family, language, faith, and community. If a counselor's approach conflicts with your family's beliefs or rituals, that mismatch matters. Good support makes room for who your family is.
What to Expect in a Bereavement Session
The first contact is usually much gentler than people expect. It often starts with a phone call or intake conversation, not a deep emotional dive. The goal is to understand who died, what has been hardest, what kind of support you're looking for, and whether the service is the right fit.

The first conversation
You usually won't be expected to tell the whole story at once. Most bereavement specialists know that the beginning can feel foggy, repetitive, or emotionally uneven.
The conversation may cover:
- Who the person was to you: spouse, parent, sibling, child, partner, or friend
- What the past weeks or months have felt like: sleep, eating, work, school, family strain
- What worries you most: anniversaries, being alone, your children, or feeling unable to cope
- What support sounds tolerable: private sessions, a group, occasional check-ins, or family meetings
What happens during sessions
Sessions are usually paced to the person, not to a script. Some days you may talk mostly about the death. Other days you may talk about the kitchen table, the empty side of the bed, a holiday, or the irritation of being told to “stay strong.”
Counseling may include remembering the person fully. That means not only their death, but their habits, voice, difficult traits, routines, and place in the family. It may also include coping strategies for getting through evenings, handling paperwork, or responding to well-meaning people who say the wrong thing.
You don't need to arrive with a lesson, insight, or tidy story. Showing up as you are is enough.
What a session should feel like
A bereavement session should feel respectful, unhurried, and nonjudgmental. You should not feel pushed to perform grief in a certain way. You also shouldn't feel dismissed if your distress is affecting your ability to function.
That balance matters. Good support makes room for grief as a human experience while also paying attention to signs that more specialized treatment may be needed.
Grief Support at Central Coast VNA & Hospice
Hospice bereavement support is often misunderstood as a few condolence calls after the death. In reality, major U.S. hospice programs commonly provide a structured bereavement service for up to 13 months after a loss, with support that may include outreach, groups, memorial events, face-to-face counseling, and referral when a person's needs go beyond routine bereavement follow-up (structured hospice bereavement services and triage).
That model is practical because grief doesn't unfold on a tidy schedule. The first holidays, birthdays, and seasonal anniversaries often land after the immediate shock has faded.
 bereavement care program and supportive community resources." />
bereavement care program and supportive community resources." />How hospice-based support is different
Hospice bereavement care is usually tiered. Lower-intensity support is available to most families, while people with signs of more serious difficulty may need specialty mental health referral rather than routine follow-up alone.
In practical terms, that can include:
- Universal outreach: phone calls, mailings, memorial gatherings, and information
- Moderate support: support groups, one-on-one bereavement conversations, and check-ins over time
- Higher-need response: clearer assessment and referral when grief is complicated by severe impairment, substance misuse, or other mental health concerns
This approach respects the fact that families don't all need the same thing.
What families on the Central Coast may look for
In Monterey County, Santa Cruz County, San Benito County, and nearby communities such as Salinas and Hollister, families often want more than a generic list of grief resources. They want to know who can help, whether support includes children or teens, whether Spanish-language support is available, and what happens if one family member wants counseling while another wants a group or pastoral support.
One local option is Central Coast VNA & Hospice, which provides hospice-related bereavement support through an interdisciplinary team that includes nurses, therapists, social workers, chaplains, and volunteers, with grief support as part of family support after hospice. For many families, the value of a hospice-based program is that it can start with simple contact and build only as needed.
That's often the right pace after a loss.
Frequently Asked Questions About Grief Support
Is my grief normal
Grief is personal, and it can be messy. You may feel significant sadness one day and oddly practical the next. You may miss the person intensely and still feel relief that their suffering ended. Those mixed reactions are common.
The better question is often not “Is this normal?” but “Is this becoming too hard to carry alone?”
How do I know what kind of support to choose
Start with your current need, not what sounds most impressive.
- If you need privacy, individual counseling may fit best.
- If you feel isolated, a group may help more than one-on-one sessions.
- If the household is struggling, family support may be more useful than separate counseling.
- If a child or teen is grieving, look for age-appropriate support rather than expecting them to fit into an adult model.
How much does grief counseling cost
Coverage and out-of-pocket costs vary by setting, eligibility, and insurance. Hospice-based bereavement support may be included for families who received hospice services, while community counseling and private therapy vary.
The simplest next step is to call and ask what is offered, who is eligible, and what coverage may apply. Avoid assuming that all grief services work the same way.
How can I help a grieving relative or friend
Stay simple and consistent. Most grieving people don't need perfect words. They need steadiness.
Try this:
- Be specific: offer a meal, a ride, school pickup, or help with forms
- Use the person's name: many grieving families need to hear their loved one remembered
- Keep checking in: support often drops off while grief is still intense
- Don't force a timeline: grief doesn't end because the calendar moved
When should I reach out for bereavement couseling
Reach out when you're wondering whether you should. You do not need to wait until things fall apart. If grief is disrupting daily life, straining your relationships, or leaving you unsure how to keep going, a conversation about bereavement couseling is reasonable and often helpful.
If you're looking for local guidance after a loss, VNA and Hospice serves families across Monterey County, Santa Cruz County, San Benito County, and South Santa Clara County. You can contact the team at 5 Lower Ragsdale Dr., Monterey, CA 93940, or call (831) 372-6668 to ask about hospice bereavement support, eligibility, and other grief resources in the community.

Palliative Care Meaning: A 2026 Guide to Family Support
Quick Answer
At many kitchen tables across Monterey and Santa Cruz counties, this is the moment families reach. A new diagnosis has changed the routine, symptoms are harder to control, and everyone is trying to help while feeling unsure what kind of support to ask for.
Palliative care means specialized medical support for people living with a serious illness, with the goal of improving day-to-day quality of life for both the patient and the family. It helps with symptom relief, emotional stress, and practical concerns, and it can begin early, even while treatments to cure or control the illness are still going on.
A simple way to understand it is this. Palliative care works like an extra layer of support added to the care already in place. It does not replace your doctors. It helps the whole plan feel more manageable.
For families on the Central Coast, that support often feels more personal when it comes from a local nonprofit team that knows the community. CCVNA serves families across Monterey and Santa Cruz counties with a human-centered approach, including bilingual support for families who feel more comfortable discussing care in Spanish and English.
If your loved one seems more uncomfortable, more tired, or more overwhelmed than before, asking about palliative care is a reasonable next step. Many families look up the palliative care meaning because they want relief, clearer guidance, and care that sees the person, not only the illness. If anxiety is already part of what your family is carrying, these anxiety learning resources may also help you put words to what you're feeling.
The True Palliative Care Meaning A Focus on Quality of Life
At a kitchen table, this is often the question underneath all the others. "What does palliative care mean for us right now?"
The clearest answer is this. Palliative care is specialized medical support for people living with a serious illness, focused on easing symptoms, lowering stress, and helping daily life feel more livable for both the patient and the family.

It treats the whole person
Serious illness rarely stays in one lane. Pain can affect sleep. Poor sleep can worsen anxiety. Anxiety can make breathing feel harder, make meals less appealing, and leave families feeling tense and unsure. Before long, the illness is shaping the whole day.
Palliative care steps into that full picture. It works like an extra set of skilled hands focused on comfort, communication, and support. That may include pain relief, help with nausea or fatigue, support for low mood, clearer conversations about care choices, and guidance for family members who are carrying a lot.
For families in Monterey and Santa Cruz counties, that support can feel more grounded when it comes from a local nonprofit team that knows the community. CCVNA brings a human-centered approach to palliative care, including bilingual support for families who want to talk through symptoms, goals, and next steps in Spanish or English.
It can begin earlier than many families expect
One of the biggest points of confusion is timing. Families often worry that asking for palliative care means giving up on treatment.
It does not.
A person can receive palliative care while also getting treatment for cancer, heart disease, lung disease, kidney disease, or another serious condition. The purpose is to make the road easier to travel. If curative or disease-directed treatment is the main engine, palliative care is the suspension system that helps absorb some of the bumps.
That matters because suffering often starts well before the end of an illness. Symptoms, side effects, and hard decisions can build up early, even when treatment is still active.
Quality of life is the point
Quality of life can sound vague until you put it into everyday terms. It may mean getting through a meal without pain. It may mean having enough energy to sit on the porch with family. It may mean fewer panicked nights, better sleep, or a plan that finally makes sense.
Sometimes families need support for their own stress too. If worry has become part of daily life, these anxiety learning resources may help put words to what you are feeling.
If you want a clearer picture of how this kind of support helps at home, in clinics, and during treatment, this guide to the benefits of palliative care explains what families on the Central Coast can expect.
Who Benefits from Palliative Support?
Palliative support isn't limited to one age group or one diagnosis. It helps people whose illness has started to affect comfort, daily function, or peace of mind.
That includes people living with cancer, heart disease, chronic lung disease, kidney failure, Parkinson's disease, Alzheimer's disease, stroke, diabetes, and other serious conditions. The need often becomes clearer when symptoms begin to stack up and home life starts revolving around medical problems.

Signs a person may benefit
Sometimes the best clue is not the diagnosis. It's the day-to-day experience.
A person may benefit from palliative care if they are:
- Living with ongoing symptoms like pain, shortness of breath, fatigue, nausea, or trouble sleeping
- Going to the hospital or ER often because symptoms keep flaring up
- Feeling overwhelmed by treatment choices or unsure what matters most now
- Needing more support at home with communication, planning, or emotional strain
Palliative care addresses a documented group of 8 to 12 concurrent symptoms, including pain, depression, shortness of breath, and fatigue. Early integration can improve symptom burden scores by 30% to 40%, according to Get Palliative Care.
It's not only for cancer
One of the biggest misunderstandings is that palliative support is mainly for cancer. In real life, many people who need it are living with chronic illnesses that gradually become harder to manage.
Think about an older adult with COPD who gets winded walking to the bathroom. Or someone with advanced heart failure who keeps swelling, losing sleep, and returning to the hospital. Or a family trying to support a parent with dementia who can no longer explain discomfort clearly. These are common situations where palliative care can help.
Serious illness often brings grief before a death ever occurs. Some families also look for outside emotional support, and resources like Interactive Counselling Kelowna grief therapy can be useful when anticipatory grief is part of the picture.
For older adults with chronic illness, this guide to palliative care for seniors may answer some of the next questions families usually have.
Palliative Care vs Hospice What is the Difference?
A family on the Central Coast may hear both terms during the same stressful week. One clinician says palliative care could help now. Another mentions hospice if the illness keeps progressing. It is easy to hear those words and assume they mean the same thing, or worse, that both mean giving up. They do not.
The clearest way to understand the difference is to focus on timing and goals.
Palliative care supports people living with a serious illness at any stage. Its job is to ease symptoms, lower stress, and help patients and families make care decisions that fit their values. A person can receive palliative care while still getting treatments meant to control disease, extend life, or even cure it.
Hospice care is for a later stage, when the focus shifts fully to comfort rather than cure. At that point, the care plan centers on relief, dignity, and support through the end of life.
A simple comparison helps:
| Factor | Palliative Care | Hospice Care |
|---|---|---|
| Who it's for | People living with a serious illness | People nearing the end of life with a terminal diagnosis |
| When it can begin | At any stage of serious illness | When curative treatment is no longer the goal |
| Main focus | Symptom relief, support, communication, and quality of life | Comfort, dignity, and support at the end of life |
| Can it happen with treatment? | Yes, alongside treatment meant to cure or control illness | Hospice generally begins when treatment goals shift away from cure |
| Family support | Yes | Yes |
One way to picture it is this. Palliative care works like an added layer of support wrapped around medical treatment. Hospice is the care plan when that treatment chapter has closed and comfort becomes the full priority.
That distinction matters to families in Monterey and Santa Cruz counties because early support often brings relief sooner. A local nonprofit team like CCVNA can help with pain and symptom concerns, family meetings, emotional support, and practical guidance in the home. For bilingual families, having support in the language spoken around the kitchen table can change the whole experience. Questions get answered more clearly. Fear settles down. Everyone understands what to expect.
Confusion also happens because both types of care treat the whole person, not just the diagnosis. Both care for families as well as patients. Both may include help with anxiety, shortness of breath, spiritual concerns, caregiving strain, and hard conversations about what matters most.
Grief can begin long before death. Some families also benefit from outside emotional support such as Interactive Counselling Kelowna grief therapy while they process anticipatory grief and caregiver stress.
If you want a fuller side by side explanation, CCVNA offers a plain-language guide on the real difference between hospice and palliative care.
Your Palliative Care Team Members and Their Roles
A good palliative care team works like a circle around the patient and family. Each person brings a different kind of help, so one hard day does not have to be carried by one clinician alone.
Serious illness often affects many parts of life at once. Pain may flare up. Sleep may fall apart. A spouse may be exhausted. Adult children may disagree about what should happen next. Someone may be scared to ask, "What are we preparing for?" Palliative care brings together the people who can address each of those needs in a coordinated, human way.

Who may be on the team
The exact mix depends on the person's condition, goals, and home situation. At a local nonprofit like CCVNA, the team is built around what the patient and family need, not a one-size-fits-all checklist. For families across Monterey and Santa Cruz counties, that can also include bilingual support that helps everyone understand the plan clearly and ask questions in the language spoken at home.
Team members often include:
- Nurses who check symptoms, watch for changes, explain medications, and help families know what to report
- Therapists who help with strength, balance, movement, safety, and daily tasks when those needs are part of the care plan
- Social workers who support coping, family communication, care planning, and access to community resources
- Chaplains who offer spiritual care, quiet presence, and space for questions about meaning, worry, or grief
- Volunteers who provide companionship and reduce isolation
What each role can feel like in real life
Families are often relieved to learn that palliative care is not only about symptom checklists. It is also about having the right person step in at the right moment.
A nurse might notice that shortness of breath is getting worse and help the family understand what changes to watch for. A social worker may sit at the kitchen table and guide a difficult family conversation that has been avoided for weeks. A chaplain may spend time with a patient who is not asking for religious answers, but does want someone to stay present with fear and uncertainty.
For a person living with heart failure, lung disease, cancer, or another serious illness, these roles connect. The team shares information, listens for what matters most, and adjusts the plan as needs change. That is what helps care feel more steady and less chaotic.
Some families say their first moment of relief comes when they realize they no longer have to figure everything out by themselves.
If you want a clearer picture of how clinical care and comfort support work together at home, this article on whole-person skilled nursing support at home explains that connection in plain language.
How Palliative Care is Covered by Insurance
This is one of the first questions families ask, and it's a reasonable one. People want help, but they also need to understand what services may be covered.
Coverage depends on the person's insurance plan, diagnosis, eligibility, and the specific services being provided. In many cases, palliative care is covered in a way that is similar to other specialist medical services, but the details can vary.

What families should ask
When you call an agency or speak with a medical office, ask these questions plainly:
- Is palliative care covered under this plan?
- Do I need a physician referral or order?
- Which visits or services are included?
- What will you help us verify before care begins?
Medicare, Medi-Cal, and private insurance coverage can differ from one person to the next. It helps to talk with someone who can review the plan and explain what applies to your situation.
For families already trying to sort through home-based benefits, this guide to Medicare home care eligibility may help clarify some of the basics.
How to Start a Conversation About Palliative Care
Most families don't begin with perfect wording. They begin with concern. A daughter notices her father isn't bouncing back after another hospitalization. A spouse sees that pain and fatigue are taking over the day. Someone says, "We need more help than we're getting."
That is enough to start.
Questions you can ask a doctor
You can say:
- Can we request a palliative care consultation?
- Who can help with symptom management at home?
- My family member is struggling. What extra support is available?
- Can we discuss comfort, goals, and what to expect?
A family doesn't have to wait for a crisis to bring this up. In fact, earlier conversations are often calmer and more useful.
Language matters on the Central Coast
For many families in Monterey County and nearby communities, language and culture affect whether palliative support feels approachable. In California, Latino patients with advanced cancer are less likely to receive palliative care referrals, and language barriers were cited in 62% of cases, according to this discussion of palliative care access and language barriers.
That matters in places like Monterey, Salinas, Santa Cruz County, and Hollister, where families may want conversations in Spanish and may make decisions together as a family unit. Bilingual support can make these discussions clearer, less intimidating, and more respectful.
If something feels unclear, ask for the explanation again in the language and wording your family understands best.
Frequently Asked Questions About Palliative Care
Does palliative care mean my loved one is dying?
No. Palliative care can begin at any stage of a serious illness. Many people receive it while continuing treatment for their condition.
Who qualifies for palliative care?
A person may qualify if they are living with a serious illness and dealing with symptoms, stress, or complicated medical decisions. Eligibility depends on the medical situation and the provider's program.
Can palliative care happen at home?
Yes, in many cases it can. Home-based support can be especially helpful for people with mobility limits, frequent symptoms, or difficulty getting to appointments.
Do we need a doctor to bring it up first?
Not always. Families can ask the primary doctor, specialist, hospital team, or a local provider directly about how to get started.
Will palliative care replace the patient's other doctors?
No. Palliative clinicians usually work alongside the patient's existing doctors. The idea is to add support, communication, and symptom management, not take over everything.
Is palliative care only for older adults?
No. While many older adults benefit from it, palliative care is for people of any age living with a serious illness.
Call to Action
If you're still sorting out the palliative care meaning for your family, it may help to talk it through with someone who does this every day. A calm conversation can make the next step feel much more manageable.
If you live in Monterey County, Santa Cruz County, San Benito County, or South Santa Clara County and want to talk with a local nonprofit team about palliative care, contact VNA and Hospice at (831) 372-6668 or visit 5 Lower Ragsdale Dr., Monterey, CA 93940. You can also learn more at ccvna.com.