Direct Answer: Comfort-focused care means prioritizing a person’s quality of life — managing pain, reducing symptoms, and supporting emotional well-being — rather than pursuing curative treatment. It applies in palliative care, hospice, and serious illness support.
Families across Monterey County hear the phrase “comfort-focused care” at some point during a serious illness — often from a doctor, a discharge planner at Community Hospital of the Monterey Peninsula, or a nurse after a difficult diagnosis. And most of the time, they nod along without being entirely sure what it means.
That’s not their fault. The phrase gets used loosely, and it carries emotional weight that makes people hesitant to ask follow-up questions. Does it mean treatment is stopping? Does it mean the end is near? Does choosing comfort mean giving up?
The honest answers are no, not necessarily, and never. What comfort-focused care actually describes is a shift in what the care team is working toward — and understanding that shift is one of the most useful things a family can know when they’re navigating serious illness.
The Difference Between Curing and Caring
Most of the medical system is built around fixing things — treating infections, removing tumors, repairing damage. That approach works well when the problem is solvable. But for many people living with a serious or advanced illness, cure isn’t always on the table. And that’s when the goals of care need to shift.
Comfort-focused care means the primary goal becomes quality of life — not length of life, not test results, not disease management for its own sake. It asks: what does this person need to feel as well as possible, right now, in the life they’re actually living?
For a 78-year-old in Salinas managing congestive heart failure, that might mean adjusting medications to reduce breathlessness rather than pursuing another hospitalization. For someone in Pacific Grove with advanced cancer, it might mean focusing on pain control, sleep, and being present with family rather than continuing chemotherapy with significant side effects.
This isn’t a lesser form of care. In many cases it requires more clinical attention, not less — because managing complex symptoms at home takes real skill. What does a skilled nurse actually do on a home visit? is a question worth asking, because the answer might surprise families who assume comfort care is just “keeping someone comfortable” in a passive sense.
Palliative Care vs. Hospice — Where Comfort Care Lives
Two programs put comfort-focused care into practice: palliative care and hospice. They’re related, but they’re not the same thing, and the difference matters a lot to families trying to make decisions.
Palliative care can start at any point after a serious diagnosis — even while a person is still pursuing curative treatment. It layers on top of whatever else is happening medically. A person can be receiving chemotherapy and palliative care at the same time. The palliative care team focuses on symptoms, emotional support, care planning, and helping the family understand what’s ahead.
Hospice care is specifically for people who have decided — usually alongside their physician — to stop pursuing curative treatment and focus entirely on comfort. Medicare’s hospice benefit requires a physician to certify that the patient’s life expectancy is six months or less if the illness follows its expected course. But it’s important to know: people can live on hospice longer than six months, and they can also choose to leave hospice if their condition stabilizes.
Here’s how families often describe the distinction:
- Palliative care: still fighting the illness, but with a team helping manage the burden of it
- Hospice care: no longer trying to cure the illness, with a team focused entirely on comfort and quality of life
Both involve nurses, therapists, social workers, chaplains, and volunteers working together. Neither one is about doing less. For a deeper look at what palliative care actually means for families, it’s worth reading through the specifics before making any decisions.

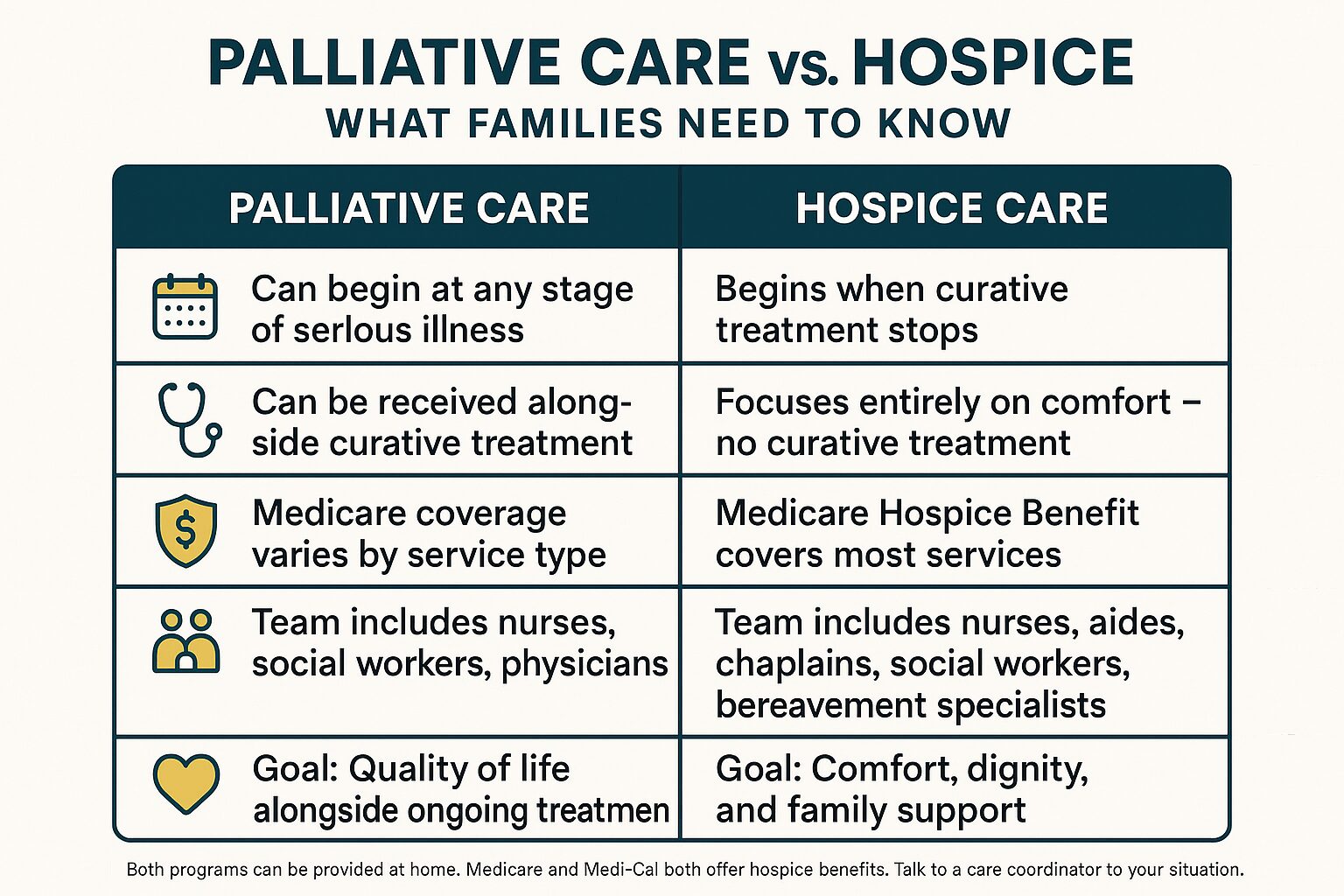
Palliative Care vs. Hospice: A Side-by-Side Look
This comparison helps families quickly see how the two programs differ in terms of goals, timing, and what Medicare covers.
When Families Actually Ask About It — and Why They Wait
In Monterey County, families often ask about comfort-focused care later than they wish they had. This comes up again and again — not because families don’t care, but because the system doesn’t always make it easy to know when to bring it up.
There’s no single right moment. But there are signals worth paying attention to:
- A loved one has been hospitalized two or more times in the past six months for the same condition
- Treatments are causing significant side effects without clear benefit
- A physician has mentioned that the illness is “not responding” or is “progressing”
- The person with the illness has expressed that they feel tired of treatment
- A family member has had to step back from work or their own life to manage care
- Discharge planners at the hospital have raised the question of home-based support
None of these signals means hospice is the immediate answer. But they do mean the conversation is worth having. What families in Monterey wish they’d known sooner about home care often includes wishing they had asked about comfort-focused options earlier — not because it would have changed the outcome, but because it would have reduced suffering in the meantime.
And asking doesn’t commit anyone to anything. It’s a conversation, not a contract.
What Comfort-Focused Care Can Look Like at Home
Comfort-focused care is practical, not abstract. Here’s a plain-language look at what different team members actually do in the home.
| Team Member | What They Focus On | How Often They Visit |
|---|---|---|
| Registered Nurse (RN) | Pain assessment, medication management, wound care, symptom monitoring | Several times per week, or as needed |
| Licensed Vocational Nurse (LVN) | Medication review, vital signs, day-to-day symptom support | Coordinated with RN schedule |
| Medical Social Worker | Emotional support, care planning, connecting families to local resources | Weekly or as needed |
| Chaplain | Spiritual care and emotional presence for patient and family | As requested or scheduled |
| Hospice Aide | Personal care, bathing, comfort routines | Daily or several times per week |
| Bereavement Specialist | Grief support for family members — before and after the patient’s passing | Ongoing, continues after death |
| Volunteers | Companionship, respite for family, errands, reading aloud | Flexible, scheduled with the family |
How Medicare and Medi-Cal Actually Cover This
One of the biggest reasons families hesitate to ask about comfort-focused care is cost. The assumption is that it’s expensive, or that insurance won’t cover it. In most cases, that assumption is wrong.
Medicare’s Hospice Benefit covers virtually all hospice-related services for eligible patients — nursing visits, medications related to the terminal diagnosis, medical equipment like hospital beds and wheelchairs, and support from the full care team including chaplains and bereavement specialists. The patient typically pays nothing out of pocket for these services.
Medi-Cal also provides a hospice benefit with similar coverage. And for veterans living in Salinas, King City, Hollister, or elsewhere in the region, VA benefits may cover home-based comfort care as well.
Palliative care coverage is more variable. It depends on the specific services and how they’re billed. But many palliative care visits — particularly those involving Registered Nurses or social workers — are covered under standard Medicare home health benefits when a physician orders them.
If you’re uncertain what would be covered in a specific situation, a care coordinator can walk through the details before any commitment is made. What families need to know about Medicare coverage for home care covers many of the common questions families ask.
Frequently Asked Questions About Comfort-Focused Care
Does choosing comfort-focused care mean we’re giving up?
No. Choosing comfort-focused care means changing the goal — from trying to cure an illness to making sure the person with that illness feels as well as possible. Many families who’ve made that shift say it was the most loving decision they ever made, not a defeat. How families describe the moment they chose hospice is worth reading if you’re wrestling with this question.
Can someone receive palliative care while still getting chemotherapy or other treatment?
Yes. Palliative care does not require stopping treatment. It works alongside whatever treatment a person is receiving. The palliative care team focuses on managing symptoms — nausea, pain, fatigue, anxiety — that treatment often causes, as well as supporting the family through a difficult time.
What happens if someone on hospice starts to get better?
They can leave hospice. There’s no penalty and no paperwork punishment for choosing to resume curative treatment if a person’s condition improves. Some people stabilize, leave hospice, and re-enroll later. The hospice benefit under Medicare can be used more than once.
How do we know if our family member qualifies for hospice?
Qualification requires a physician to certify that the patient’s life expectancy is six months or less if the illness follows its expected path. The patient (or their representative) also needs to agree to focus on comfort rather than cure. A care coordinator or the patient’s physician can help determine eligibility — it’s a conversation, not a complicated application process.
Can comfort-focused care happen at home, or does it require a facility?
Most comfort-focused care — including both palliative care and hospice — is delivered at home. For families in Monterey County, that means a patient can stay in their own house, with their own routines and the people they love around them, while still receiving skilled clinical support. Facility-based hospice exists but is typically reserved for symptom crises that can’t be managed at home.
What support does the family get — not just the patient?
Quite a bit. Hospice care includes medical social workers for emotional and practical support, chaplains for spiritual care, and bereavement specialists who work with the family both before and after a patient’s passing. Bereavement support continues for at least 13 months after the death of a loved one under the Medicare Hospice Benefit. That’s not a minor detail — grief doesn’t follow a schedule, and having a bereavement specialist available during that time makes a real difference.
Still Have Questions About What This Could Look Like for Your Family?
Central Coast VNA & Hospice has been supporting families across Monterey County — from the Peninsula to Salinas to King City — since 1951. If you’re trying to understand whether comfort-focused care makes sense for your situation, a care coordinator can talk through the specifics without pressure or obligation. Call 831-372-6668 or visit ccvna.com to start the conversation.