Direct Answer: Needing help at home and needing a facility are two very different things. Most families in Monterey County don’t need a facility — they need the right support brought to where their loved one already lives.
When a parent’s health starts to slip, the mind goes straight to the hardest question: do we need to move them somewhere? It’s one of the most emotionally loaded decisions a family can face — and in Monterey County, it’s a question thousands of families work through every year without a clear roadmap.
But here’s what often gets missed: needing help is not the same as needing a facility. A lot of families assume those are the only two options — either you manage everything yourself, or you start looking at skilled nursing facilities in Salinas or memory care units on the Peninsula. There’s a wide middle ground that most people never fully explore.
This guide is for families trying to understand what home-based care can actually handle — and where the real line is between that and facility-level care. No sales pitch. Just a clear-eyed look at what the options actually mean.
What ‘Needing Help’ Actually Looks Like
Most families recognize something is off before they can name it. Dad is slower getting up. Mom missed two doses of her blood pressure medication. A fall happened — or almost happened. These are signals, but they don’t automatically mean a facility is the answer.
Home-based support exists precisely for this stage. Skilled nursing visits, physical therapy, medication management, wound care after a surgery — these are all services that can come to your loved one’s home in Monterey, Salinas, Hollister, or King City without uprooting their life.
The kinds of situations that respond well to home-based care include:
- Recovery from a hospital stay or surgery
- Managing a chronic illness like heart failure, COPD, or diabetes
- Wound care that requires a Registered Nurse’s assessment
- Physical therapy after a hip or knee replacement
- Medication reviews and adjustments supervised by a clinician
- Early or moderate cognitive changes where the person is still safe at home
None of these automatically require a facility. And for many families, understanding what home care can realistically provide changes the entire conversation.
The goal of home-based skilled care isn’t to avoid hard decisions indefinitely — it’s to make sure families aren’t making those hard decisions prematurely, before they’ve tried what’s actually available to them.

Where the Real Line Is: When a Facility Becomes Necessary
Home-based care has real limits, and it’s important to name them honestly.
A facility becomes the right answer when the level of supervision or medical complexity exceeds what can be safely managed — even with daily visits from nurses and therapists. 24-hour supervision, certain types of wound care requiring constant monitoring, or situations where a person can no longer be left alone safely for any stretch of time are examples where the home setting may no longer be appropriate.
Some specific indicators that point toward facility-level care:
- The person is a fall risk who cannot be left unsupervised at any point during the day or night
- They require ventilator support or IV therapy that can’t be managed intermittently
- Behavioral symptoms of dementia — aggression, wandering, or severe disorientation — have become unsafe for everyone in the home
- The primary family support in Salinas, Pacific Grove, or wherever they live has reached a point of physical or emotional exhaustion that creates a safety risk
- Round-the-clock hands-on assistance with eating, bathing, and repositioning is required every few hours, not just once or twice a day
These are specific, clinical thresholds. And reaching one of them doesn’t mean failure — it means the situation has changed, and the right support has to change with it.
For families navigating serious illness who haven’t reached that threshold, palliative care at home often provides the symptom management and care coordination that keeps people safely in place far longer than families expect.
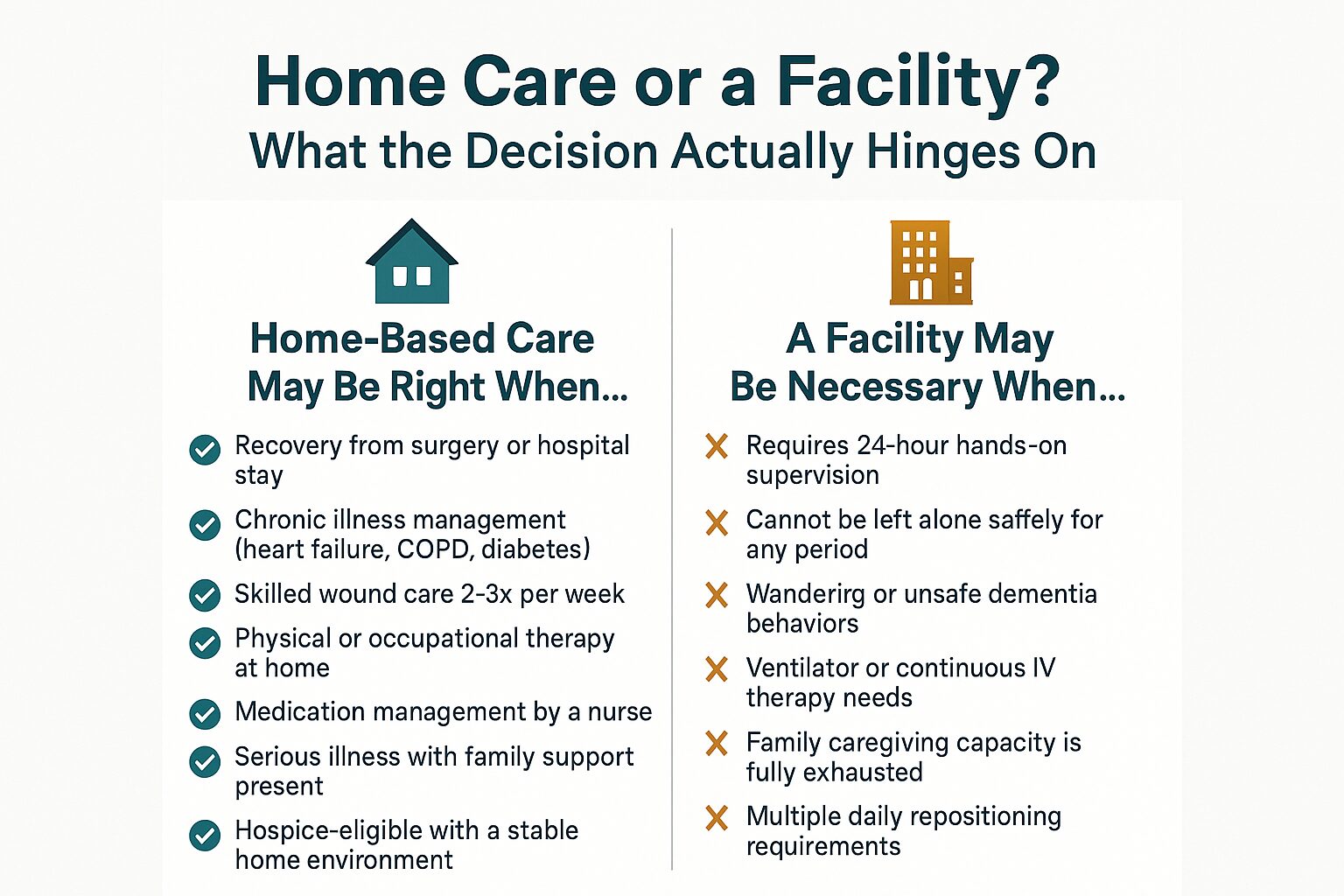
Home Care vs. Facility Care: How the Decision Actually Works
This breakdown shows the key factors that separate home-based care from facility-level care — and what the decision hinges on for most Monterey County families.
What Medicare Actually Covers at Home — and What It Doesn’t
One reason families jump to facility thinking is cost uncertainty. They don’t know what Medicare covers at home, so they assume a facility is the only structured option.
Medicare covers skilled home health services when a physician certifies that the patient is homebound and needs skilled nursing, physical therapy, occupational therapy, or speech therapy. That coverage is meaningful — it includes Registered Nurse visits, Licensed Vocational Nurse visits, therapy sessions, and Medical Social Worker support, all without a copay under traditional Medicare Part A and B.
What Medicare does not cover at home:
- Custodial care — help with bathing, dressing, and meals — unless it accompanies a skilled service
- 24-hour home supervision
- Long-term personal care without a skilled medical need
Medi-Cal can fill some of those gaps for qualifying patients in Monterey County. And for families facing end-of-life situations, the Medicare Hospice Benefit covers a wide range of services — nursing, aide support, medications related to the terminal diagnosis, chaplain visits, and bereavement support — with no cost-sharing for Medicare beneficiaries.
Veterans receiving care through VA benefits may have additional options worth exploring through a Medical Social Worker.
For a closer look at how coverage works, this breakdown of Medicare home health coverage walks through what’s included and how to know if a patient qualifies.
Home Care vs. Facility Care: A Side-by-Side Look
This table gives families a concrete comparison of what each setting typically provides and what it costs in the Monterey County area.
| Factor | Home-Based Skilled Care | Skilled Nursing Facility |
|---|---|---|
| Setting | Patient’s own home | Residential facility |
| Medicare coverage | Covered when homebound + skilled need certified | Covered for short-term rehab stays (up to 100 days) |
| Typical out-of-pocket cost (Monterey County) | $0 copay for Medicare-covered skilled visits | $194.50/day after day 20 (2024 Medicare rate) |
| Who provides care | RNs, LVNs, PTs, OTs, Social Workers, Aides on scheduled visits | On-site nursing staff 24 hours/day |
| Level of supervision | Intermittent — visits, not constant presence | Continuous staff availability |
| Best suited for | Recovery, chronic illness management, serious illness with family support | High-acuity needs, post-acute rehab requiring 24-hour oversight |
| Patient autonomy | Full control over environment, routine, diet | Structured facility schedule and environment |
| Hospice eligible | Yes — hospice is primarily delivered at home | Yes — hospice can be provided in facilities too |
The Conversation Families Avoid — and Why It Matters
Most families put off this conversation until something forces it — a hospitalization, a bad fall, or a crisis that lands everyone in an ER waiting room at midnight. By then, decisions get made under pressure instead of with clarity.
Having the conversation earlier — when a parent is still relatively stable — is one of the most practical things a family can do. It’s not morbid. It’s the opposite: it protects the person’s ability to stay in their own home longer, because you’ve identified what support would make that possible before a crisis strips away those options.
For families in Pacific Grove, Carmel, Hollister, or anywhere across Monterey County, knowing when to start thinking about home care is the kind of guidance that changes outcomes — not because it speeds anything up, but because it gives families more real choices.
And for those dealing with a serious illness diagnosis, palliative care is often the missing piece. It doesn’t replace treatment, and it doesn’t mean giving up. It means a team of nurses, therapists, social workers, and chaplains is actively managing symptoms and supporting the family while the patient continues receiving care.
Frequently Asked Questions About Home Care vs. Facility Care
Can someone with dementia stay at home with skilled care support?
Often, yes — for a significant portion of the illness. The determining factor isn’t the diagnosis itself but the level of supervision required and the safety of the home environment. Early to moderate dementia, where the person is not wandering or posing a physical danger, can frequently be managed at home with a combination of family involvement, skilled nursing visits, and home health aide support. When behavioral symptoms become unpredictable or dangerous, that’s when the balance shifts.
My mother just got out of the hospital. Does she automatically qualify for home health?
A hospital stay doesn’t automatically qualify someone, but it’s one of the most common pathways. Medicare requires that a physician certify the patient as homebound (meaning leaving home requires considerable effort) and that there is a skilled need — nursing, therapy, or both. Discharge planners at hospitals in Salinas or Monterey can initiate the referral before the patient even leaves.
Is hospice only for the last few days of life?
No — and this is one of the most damaging misconceptions families carry. Hospice is available when a physician certifies that a patient has a life-limiting illness with a prognosis of six months or less if the disease follows its expected course. Many patients receive hospice care for weeks or months, not just days. Families who access hospice earlier consistently report better pain control and more time to focus on what matters. You can read more in this guide to hospice care for families.
What if we can’t afford a facility but aren’t sure home care is enough?
Talk to a Medical Social Worker before making any decisions. They can assess the actual clinical picture, map out what Medicare or Medi-Cal covers, and identify realistic options — including whether the level of need actually calls for a facility at all. In many cases, families who assume they need a facility find that structured home-based care with the right clinical team covers what’s needed.
What happens to the family after a loved one passes — does support end?
Bereavement support continues after a patient’s death. Families who received hospice care have access to grief counseling and ongoing emotional support through bereavement specialists — typically for at least 13 months following the loss. Bereavement support services are also available to community members in Monterey County who didn’t receive hospice care through VNA.
Not Sure Which Direction Makes Sense for Your Family?
Central Coast VNA & Hospice has been walking alongside families in Monterey County, Salinas, Hollister, and the surrounding Central Coast since 1951 — including families facing exactly the kind of decision this article is about. A care coordinator can help you think through what your loved one’s situation actually calls for, without pressure and without guesswork. Call 831-372-6668 or visit ccvna.com to start that conversation.