Direct Answer: A skilled nurse assesses your loved one’s health, manages medications and wound care, monitors for complications, and communicates directly with their physician — all at home.
Most families in Monterey County have a vague sense that home nursing means ‘someone comes to check on Mom.’ But when you’re making real decisions about a parent recovering from surgery in Pacific Grove or managing heart failure in Salinas, ‘someone checks in’ doesn’t tell you much.
A skilled nursing visit is a medical appointment — it just happens in your living room instead of a clinic. The nurse arrives with clinical tools, a care plan, and direct communication with your loved one’s physician. What they do in that hour or so has real consequences for whether someone stays stable at home or ends up back in the hospital.
This article walks through what actually happens during those visits, what problems skilled nurses are trained to catch, and how to know whether your family’s situation fits what home health can provide.
The First Visit: More Than a Checkup
The initial home visit is longer and more detailed than follow-up visits — often 60 to 90 minutes. A Registered Nurse conducts a head-to-toe assessment that covers far more than vital signs.
They’re building a clinical picture of the patient in their actual environment. That means looking at how the person moves through their home, whether they can safely take their own medications, and what the home itself might be doing to their health — poor lighting, loose rugs, a second-floor bathroom when someone has balance problems.
For families in Monterey County, that first visit also establishes a baseline. If your parent was discharged from Salinas Valley Health or Community Hospital of the Monterey Peninsula after a hip replacement, the nurse arriving at home is working from that discharge summary and confirming that what was documented actually matches what they see in front of them. Those details don’t always line up.
By the end of the first visit, the nurse has:
– Completed a full physical assessment
– Reviewed every medication for accuracy, interactions, and adherence
– Identified safety concerns in the home
– Set goals with the patient and family
– Contacted the physician if anything needs to be addressed immediately
What Skilled Nurses Are Actually Watching For
Follow-up visits — which may happen two to three times per week depending on the care plan — are focused and clinical. The nurse isn’t just stopping by. They’re tracking specific indicators that tell them whether the patient is improving, plateauing, or heading toward a problem.
For someone recovering from cardiac surgery, that might mean monitoring fluid retention and checking whether ankles are swelling. For a patient with diabetes, it means reviewing blood sugar logs and looking at any wounds on the feet. For someone on a blood thinner after a stroke, it means watching for signs of bleeding or new neurological changes.
This kind of close monitoring is what many Monterey families didn’t realize was available at home until they needed it.
Common clinical tasks during a skilled nursing visit include:
– Blood pressure, pulse, respiratory rate, and oxygen saturation monitoring
– Wound assessment and dressing changes — including surgical incisions, pressure injuries, and diabetic ulcers
– Medication reconciliation — confirming the patient is taking the right doses at the right times, and flagging anything that changed at discharge
– IV therapy or injections when ordered by the physician
– Catheter care
– Patient and family education — teaching family members what to watch for between visits
The education piece matters more than most families expect. A skilled nurse will walk a spouse or adult child through how to recognize signs that something is wrong — what shortness of breath looks like in someone with CHF, or when a wound needs to be called in to the physician. That knowledge is what keeps people out of the emergency room at 2 a.m.
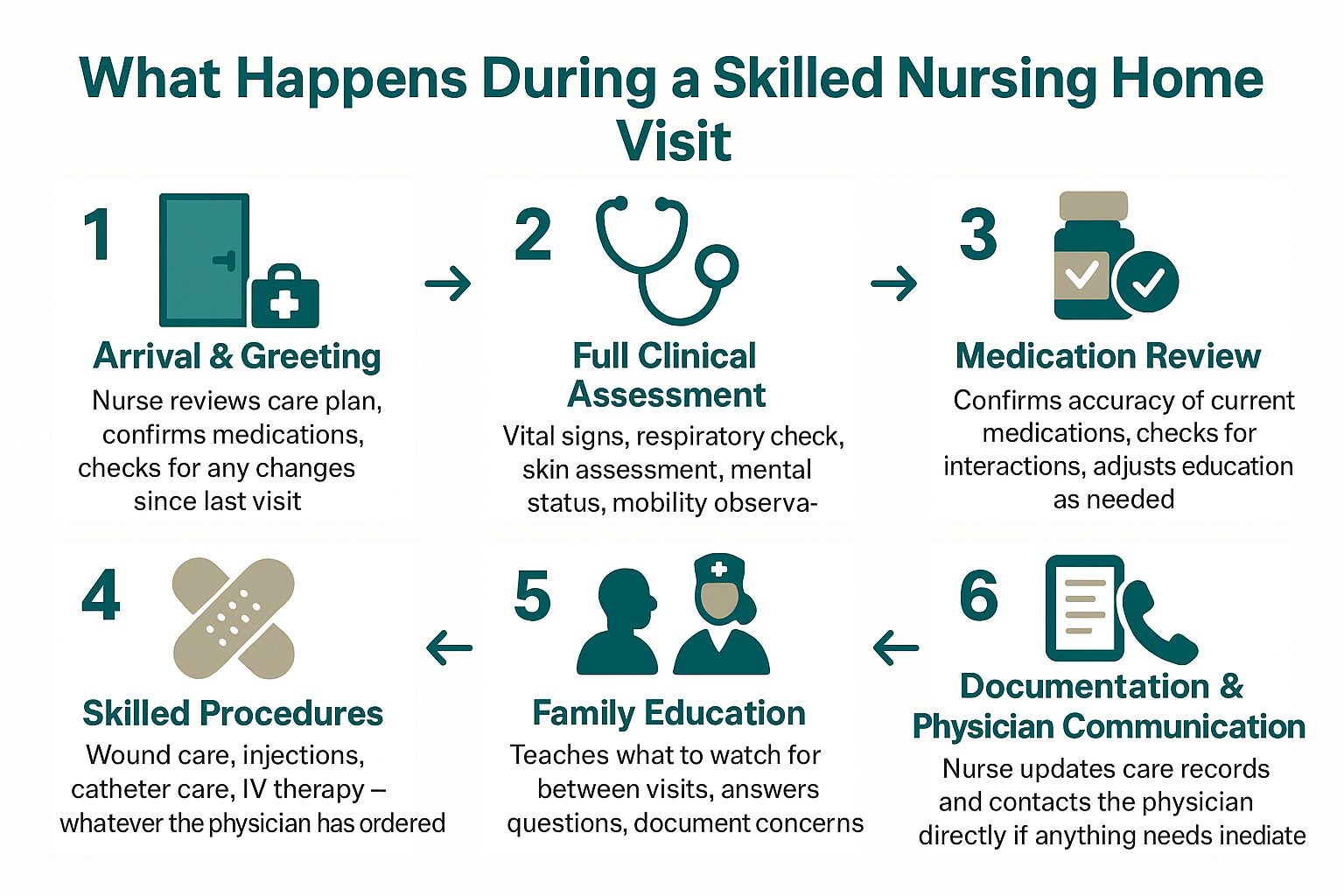
A Typical Skilled Nursing Visit: What Happens and When
This breakdown shows the general flow of a skilled nursing home visit — from arrival to documentation — so families know what to expect.
When a Nurse Notices Something the Doctor Hasn’t Seen Yet
One thing families consistently underestimate is how much clinical information a home nurse captures that a clinic visit never would.
In a physician’s office, a patient is there for 15 to 20 minutes, often in their best condition — dressed, alert, accompanied by a family member who’s managing the situation. At home, a nurse sees how that same person actually functions. Do they forget to take their medication until reminded? Do they struggle to get up from the couch? Are they eating?
For patients managing chronic illness in communities like King City or Hollister — where the nearest specialist might be an hour away — this kind of close, repeated observation is often what catches a decline early enough to do something about it.
Skilled nurses are required to communicate changes to the ordering physician. If a patient’s weight jumps 5 pounds in 48 hours — a common early warning sign of fluid retention in heart failure patients — the nurse calls the physician that day. That call may result in a medication adjustment that prevents hospitalization. That’s not a routine checkup. That’s active clinical management.
It’s also worth understanding that skilled nursing works best as part of a team. Depending on the care plan, a patient might also be receiving visits from Physical Therapists, Occupational Therapists, Speech Therapists, or Medical Social Workers — all coordinated under the same plan. Staying home as health needs change depends heavily on that kind of coordination working smoothly.
Skilled Nursing vs. Home Health Aide: What’s the Difference?
Families often confuse skilled nursing visits with home health aide services. They’re not the same thing, and insurance coverage reflects that distinction.
| Skilled Nurse (RN or LVN) | Home Health Aide | |
|---|---|---|
| Training required | Licensed RN or LVN | Certified Home Health Aide (CHHA) |
| What they do | Clinical assessment, wound care, medication management, IV therapy, physician communication | Bathing, dressing, grooming, light household tasks |
| Can administer medications? | Yes | No |
| Medicare coverage | Covered when medically necessary and homebound criteria are met | Covered only when skilled nursing or therapy is also being received |
| Who orders the visits? | Physician order required | Physician order required (as part of the broader home health plan) |
| Typical visit length | 45–90 minutes | 2–4 hours |
Does Medicare Cover Skilled Nursing at Home?
Medicare Part A covers skilled nursing visits at home when three conditions are met: the patient is considered homebound, a physician has ordered the care, and the services are provided by a Medicare-certified home health agency.
‘Homebound’ doesn’t mean bedridden. It means leaving home requires a considerable effort — using a walker, needing assistance, or risking your health by going out. Most patients recovering from surgery or managing serious illness qualify.
When those criteria are met, Medicare covers skilled nursing visits at no cost to the patient — no copay, no deductible for the home health benefit. That’s meaningful for families in Monterey County where the cost of care adds up quickly.
Medi-Cal and Veterans benefits also cover home health services, and understanding what happens when Medicare doesn’t cover everything is worth reading if your family is working through the financing piece.
One practical note: skilled nursing visits are not the same as private-pay companion care or housekeeping services. Those are separate, not covered by Medicare, and serve a different purpose. If you’re trying to figure out when home care is even the right step, starting with what Medicare covers is usually the most useful first question.
Frequently Asked Questions About Skilled Nursing Home Visits
How often does a skilled nurse visit?
It depends on the care plan and what the physician orders. Right after a hospital discharge, visits might happen three to five times per week. As the patient stabilizes, visits typically taper to once or twice a week. The frequency is always based on clinical need, not a set schedule.
Does my parent have to be bedridden to qualify for home nursing?
No. The Medicare definition of ‘homebound’ is broader than most people think. Someone who can walk short distances but finds it taxing, or who needs help getting in and out of a car, likely qualifies. A physician makes that determination based on the patient’s specific condition.
What’s the difference between a Registered Nurse and a Licensed Vocational Nurse on a home visit?
Both RNs and LVNs perform skilled nursing visits at home, but their scope of practice differs. Registered Nurses have a broader clinical scope — they conduct the initial assessment, develop the care plan, and handle more complex clinical situations. Licensed Vocational Nurses work under RN supervision and handle many of the ongoing visit tasks like wound care, medication management, and vital sign monitoring. For most families, both represent competent, trained clinical care.
Can the nurse communicate directly with my parent’s specialist in San Francisco or Stanford?
Yes. Skilled nurses document every visit and are required to report significant changes to the ordering physician — regardless of where that physician is located. If your parent sees a cardiologist in San Francisco but lives in Monterey, the home nurse coordinates with that physician by phone, fax, or electronic health record. Distance doesn’t prevent that communication.
What happens if the nurse finds something serious during a visit?
The nurse contacts the physician immediately and documents the finding. Depending on the situation, this might result in a same-day medication change, an order for lab work, or a recommendation to go to the emergency room. If the situation is life-threatening, the nurse calls 911. Home nurses are trained to triage exactly these moments — it’s one of the reasons close monitoring at home can prevent hospitalizations.
Is skilled nursing the same as palliative care or hospice?
No — though they can overlap. Skilled nursing is a medical service focused on recovery, chronic disease management, and post-hospital care. Palliative care adds a layer of symptom management and care planning for serious illness — and doesn’t require giving up other treatment. Hospice is specifically for end-of-life care. You can learn more about what palliative care actually means for families if that’s the direction your family is considering.
Questions About Home Nursing for a Family Member in Monterey County?
Central Coast VNA & Hospice has been providing skilled nursing care to families across Monterey County, Santa Cruz County, San Benito County, and South Santa Clara County since 1951. If you’re trying to sort out whether a loved one qualifies, what a care plan might look like, or what to ask their physician, a care coordinator can walk you through it without any pressure. Call 831-372-6668 or visit ccvna.com to start that conversation.