Direct Answer: After a hospital discharge, most patients need skilled medical support at home — not a nursing facility. Home health services like nursing, therapy, and medication management can start within 24–48 hours.
The discharge papers are signed. Your parent or spouse is being wheeled to the car. And now you’re thinking: what exactly happens next?
For families across Monterey County — whether you’re driving home from Community Hospital of the Monterey Peninsula in Monterey or Natividad Medical Center in Salinas — that moment can feel disorienting. The hospital felt safe. Home feels like a question mark.
Most patients are actually better served at home than in a skilled nursing facility after discharge, especially with the right support in place. This article walks you through what that transition really looks like, what Medicare typically covers, and how to tell whether your loved one’s needs can be met at home.
What ‘Discharge Planning’ Actually Means — and Why It Matters
Hospitals are required to have a discharge plan in place before a patient leaves. But in practice, families often receive that plan hours before departure — sometimes as a stack of papers, sometimes as a rushed hallway conversation with a social worker.
A discharge plan typically includes:
- A summary of the patient’s diagnosis and treatment
- A medication list, often with recent changes
- Follow-up appointment instructions
- Referrals to home health services, if ordered by the physician
- Activity restrictions and wound care instructions, if applicable
The most important thing to understand is this: a physician must order home health services. If the discharging doctor didn’t bring it up and you believe your loved one needs skilled care at home, you can — and should — ask directly before leaving the hospital.
If a home health referral is in the plan, services can often begin within 24 to 48 hours of discharge. That window matters, because the first few days at home carry the highest risk of readmission. According to Medicare data, nearly 1 in 5 Medicare patients is readmitted within 30 days of hospital discharge — most often due to medication errors, missed follow-up, or inadequate wound care monitoring at home.
Understanding what a skilled nurse actually does on a home visit can help families know exactly what to expect from those first days.

What Home Health Services Look Like in the First Weeks
Once home health is ordered, an intake assessment happens first — usually within 24 hours of the referral. A Registered Nurse or Licensed Vocational Nurse visits the home, reviews the discharge summary, assesses the patient’s condition, and develops a care plan with the treating physician.
Depending on what the patient needs, the care team may include:
- Registered Nurses (RNs) and Licensed Vocational Nurses (LVNs) for wound care, medication management, and health monitoring
- Physical Therapists for rebuilding strength and mobility after surgery or a fall
- Occupational Therapists to help patients safely perform daily tasks — bathing, dressing, cooking — in their own home
- Speech Therapists if swallowing, speech, or cognitive function was affected
- Medical Social Workers to help with care planning, community resources, and family support
Visit frequency depends on clinical need, not a fixed schedule. Someone recovering from hip replacement surgery in Salinas might have a Physical Therapist and RN visiting three to five days per week in the first two weeks, then tapering as they improve.
One thing families sometimes don’t expect: home health is episodic care, not ongoing custodial support. Clinicians come to assess, treat, and teach — not to provide daily personal care or companionship. If your family is sorting through what level of help is actually needed, the difference between needing help and needing a facility lays that out clearly.
Common Needs After Discharge — Who Addresses Them
Families often don’t know which type of clinician handles which post-discharge need. This table gives a quick reference for the most common situations.
| Post-Discharge Need | Who Addresses It | Typical Frequency |
|---|---|---|
| Wound care and surgical site monitoring | Registered Nurse (RN) or LVN | 2–5 visits/week initially |
| Medication changes and safety review | Registered Nurse (RN) | First visit, then as needed |
| Walking, balance, and strength recovery | Physical Therapist (PT) | 2–4 visits/week |
| Safe return to daily activities at home | Occupational Therapist (OT) | 1–3 visits/week |
| Swallowing or speech difficulty post-stroke | Speech Therapist (ST) | 2–3 visits/week |
| Care coordination, family support, resource navigation | Medical Social Worker | 1–2 visits total, or as needed |
| Pain and symptom management for serious illness | RN + full interdisciplinary team | Varies by care plan |
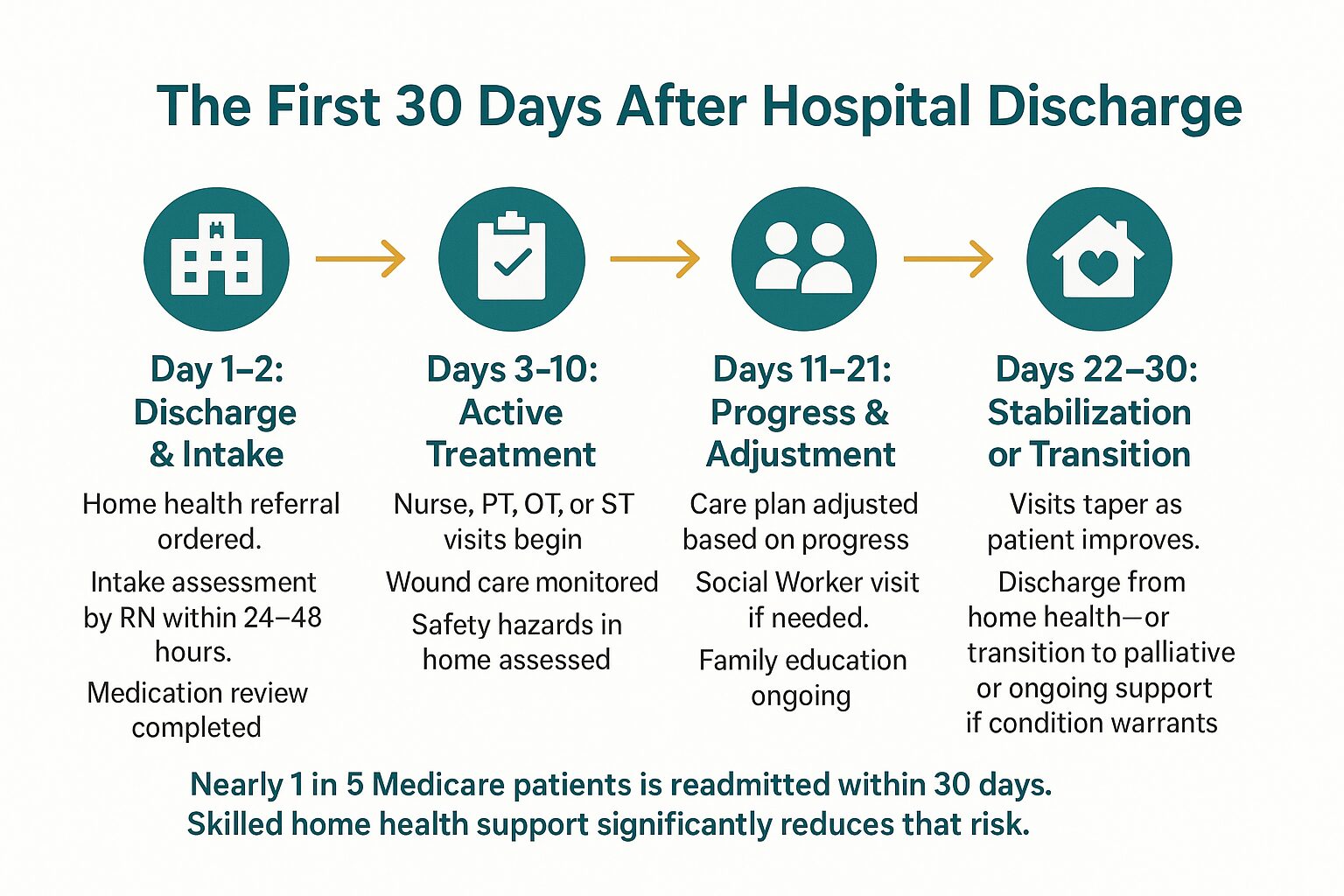
The First 30 Days at Home: What a Typical Recovery Path Looks Like
The 30 days after hospital discharge are the highest-risk window for readmission. This infographic maps out what a supported recovery typically looks like week by week.
What Medicare Covers — and Where Families Get Confused
Medicare Part A and Part B both cover home health services, but the rules trip people up. The most common misconceptions families in Monterey County run into:
Myth: Medicare only pays if you were hospitalized first.
Not true. Medicare covers home health services as long as a physician certifies that the patient is homebound and needs skilled care — regardless of whether there was a recent hospitalization.
Myth: Medicare pays for 24-hour home care.
It doesn’t. Medicare covers skilled, intermittent care — meaning clinician visits, not round-the-clock supervision or personal care assistance.
What Medicare does cover:
- Skilled nursing visits (RN or LVN)
- Physical, occupational, and speech therapy
- Medical Social Worker services
- Home health aide visits when skilled care is also being received
- Medical supplies related to the plan of care
There is no copay for Medicare-covered home health services when the agency is Medicare-certified. Families eligible for Medi-Cal may have additional benefits that cover services Medicare doesn’t reach. Veterans may have separate coverage through the VA.
For a fuller breakdown of how coverage works when Medicare doesn’t cover everything, this guide walks through your options. And if physical therapy is part of the picture, Medicare’s coverage of home physical therapy is worth reading before discharge day.
When Home Health Isn’t Enough — What Comes After
For most patients recovering from surgery or an acute illness, home health is a temporary bridge. They improve, visits taper off, and they return to managing life independently.
But for patients with a serious or progressive illness — someone with advanced heart failure, COPD, or cancer — discharge may mark the beginning of a longer road. That’s where families need to know the difference between home health, palliative care, and hospice, because these are not the same thing.
Palliative care is specialized support for serious illness that can run alongside any other treatment. It focuses on symptom management, care planning, and emotional support for both the patient and family — and patients do not have to give up curative treatment to receive it. If your family is trying to understand what this actually looks like in practice, this guide to palliative care meaning and family support is a useful starting point.
Hospice care is for patients whose illness has progressed to a point where treatment is no longer the focus — where comfort, dignity, and quality of life at home become the priority. It includes a full team: nurses, therapists, social workers, chaplains, volunteers, and bereavement specialists who support the entire family. If you’re wondering whether that conversation is worth having, The Heart of Hospice: A Guide for Families explains it without pressure.
For many families in Salinas, King City, Hollister, and across Monterey County, the question isn’t whether to ask — it’s finding a trustworthy place to start.
Frequently Asked Questions About Home Care After Hospital Discharge
How quickly can home health services start after my parent is discharged?
In most cases, an intake visit from a Registered Nurse can happen within 24 to 48 hours of discharge. If the referral is sent from the hospital before discharge, the timeline can be even shorter. The key is making sure the discharging physician submits the order before your loved one leaves the facility.
My dad was only in the hospital for two days. Does he still qualify for home health?
Possibly, yes. Medicare’s home health benefit doesn’t require a minimum hospital stay — it requires that a physician certify the patient as homebound and in need of skilled care. A two-day stay for a cardiac event or fall, for example, can absolutely qualify someone for post-discharge home nursing or therapy.
What does ‘homebound’ mean for Medicare purposes?
It means that leaving home requires a considerable effort and is medically inadvisable or physically difficult. A patient who can walk to the mailbox but cannot safely drive or travel without help typically qualifies. Your Registered Nurse or the intake team can help assess this during the first visit.
We live in King City — can home health actually reach us?
Yes. Service extends throughout Monterey County, including King City and the South County communities. Distance from the Monterey Peninsula doesn’t disqualify a patient from receiving home health, though scheduling and visit frequency may look slightly different in more rural areas.
What if my family needs more support than skilled visits can provide?
Skilled home health focuses on medical and therapeutic care, not daily personal assistance or companionship. If your loved one needs help with bathing, meals, or daily supervision beyond what clinicians provide, a Medical Social Worker can help identify community resources and non-medical support options available in Monterey County. That conversation is worth having early — not after a crisis.
Is there any cost to the family for home health under Medicare?
No copay for Medicare-covered home health services when you’re using a Medicare-certified agency. The services covered — skilled nursing, therapy, social work, home health aide visits — come at no out-of-pocket cost to Medicare beneficiaries who meet the eligibility criteria.
Questions About What Comes Next for Your Family?
Central Coast VNA & Hospice has been supporting families through exactly this kind of transition since 1951 — across Monterey County, from the Peninsula to Salinas to King City and beyond. If you’re trying to sort out what your loved one qualifies for, what Medicare covers, or whether home health is the right fit, a care coordinator can talk it through with you without pressure. Call 831-372-6668 or visit ccvna.com to start that conversation.