Direct Answer: Staying home as you age requires honest safety planning, the right medical support, and knowing when professional help — like skilled nursing or therapy — fills gaps family alone can’t cover.
Most older adults on the Monterey Peninsula will tell you the same thing when asked where they want to spend their later years: home. Not a facility. Not somewhere unfamiliar. The house they know, the neighborhood they’ve walked for decades, the kitchen where everything is exactly where they left it.
But wanting to stay home and actually being able to stay home are two different things. Families across Monterey County — from Pacific Grove to Salinas to King City — are figuring out that gap right now, often in the middle of a health crisis that didn’t leave much time to plan.
This article focuses on two things that matter most: what actually breaks down when aging at home gets hard, and what kinds of support can close those gaps before a crisis forces a different decision.
The Honest Reasons Aging at Home Gets Hard
Most families don’t run into trouble because their parent or loved one is simply “getting older.” They run into trouble when one specific thing changes — a fall, a new diagnosis, a medication that’s harder to manage, a surgery with a recovery that takes longer than expected.
In Monterey County, where many older adults live in homes built in the 1950s and 60s — stairs, narrow bathrooms, no grab bars — the physical environment is often the first problem. A house that worked fine at 65 can become genuinely hazardous by 80.
But the medical side is usually what families underestimate. Conditions like congestive heart failure, COPD, diabetes, and post-stroke recovery require ongoing clinical monitoring. Missing a medication dose or missing an early warning sign isn’t a minor inconvenience — it’s how people end up in the emergency room at Salinas Valley Health or Community Hospital of the Monterey Peninsula.
The most common breaking points look like this:
- A hospitalization that leaves someone weaker than before, with new medications and new restrictions
- A chronic condition that was manageable until it wasn’t
- A family member who was doing most of the daily support and is now overwhelmed or unavailable
- Cognitive changes that make self-care unreliable
If any of these sound familiar, you’re already in the window where knowing when to get help at home becomes a real question — not a distant one.

What Skilled Home Health Actually Does (and What It Doesn’t)
There’s a lot of confusion about what “home health” means. Many families assume it means someone comes to help with bathing and groceries. That’s not skilled home health — that’s personal care, and it’s a separate category entirely.
Skilled home health is medical care delivered in the home by licensed clinicians. That includes Registered Nurses, Licensed Vocational Nurses, Physical Therapists, Occupational Therapists, Speech Therapists, and Medical Social Workers. These are the same credentials you’d see in a hospital or outpatient clinic — just delivered where the patient actually lives.
In practice, skilled home health covers things like:
- Wound care after surgery or from a chronic condition like diabetes
- Medication management — making sure the right drugs are being taken at the right doses, watching for interactions
- Post-surgical recovery — physical and occupational therapy in the home, where the actual environment can be assessed
- Chronic disease management for conditions like heart failure, COPD, and diabetes
- Speech therapy after a stroke or neurological event
One thing that surprises many families: Medicare covers skilled home health when a physician certifies that the patient is homebound and needs skilled care. You can read more about exactly how that works for physical therapy specifically at does Medicare cover physical therapy at home.
What skilled home health does not cover is ongoing personal assistance — help getting dressed every morning, meal prep, transportation. That requires a different type of arrangement, usually paid privately or through certain Medi-Cal programs. Understanding that line early saves families a lot of frustration.
For families in communities like Hollister or King City, where driving to outpatient appointments is a real burden, receiving therapy and nursing at home removes a barrier that would otherwise mean skipping care entirely.
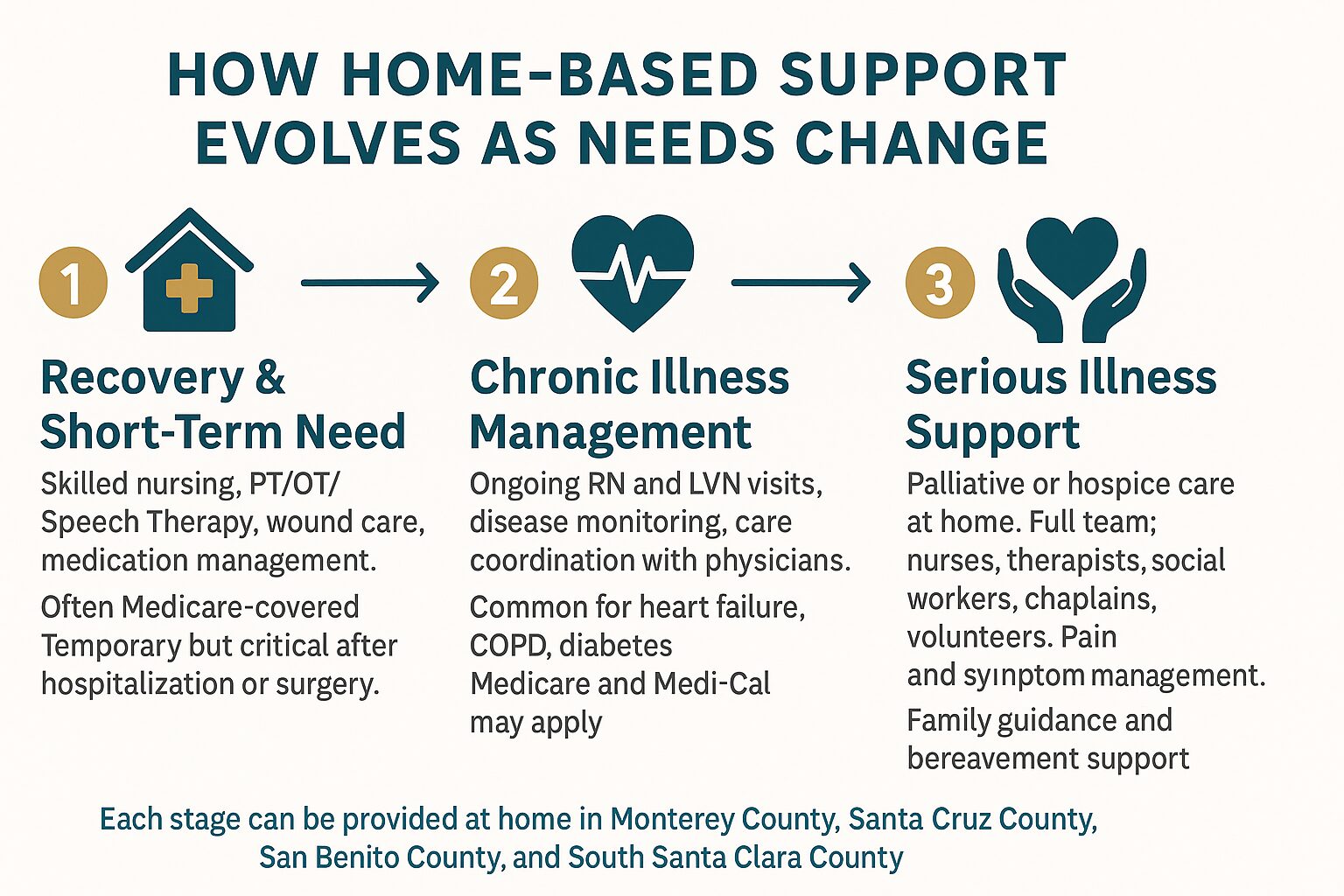
How Home-Based Support Changes Over Time
As health needs shift, the type of support that makes staying home possible shifts too. This breakdown shows how care typically evolves across different stages.
When Palliative or Hospice Care Enters the Picture
At some point, the goal of care shifts. It’s not about recovering from something — it’s about living as well as possible with something that isn’t going away.
That’s where palliative care becomes relevant. Most people have heard the term but aren’t sure what it means in practice. It doesn’t mean giving up treatment. It means adding a layer of support — symptom management, care planning, emotional support — alongside whatever other care is already happening. A Nurse Practitioner or Registered Nurse might visit the home to manage pain. A Medical Social Worker might help the family process what’s ahead. A Chaplain might sit with the patient through something a physician doesn’t have time for.
You can find a thorough explanation of what this actually looks like for families at palliative care meaning: a guide for families.
Hospice care is a separate level of care for people whose illness is terminal and who have chosen to focus on comfort rather than curative treatment. It brings an interdisciplinary team — nurses, hospice aides, chaplains, volunteers, social workers, and bereavement specialists — directly into the home. It is covered by Medicare and most Medi-Cal plans at no cost to the patient.
What hospice makes possible is something that matters deeply to most families: a loved one spending their final weeks or months at home, surrounded by familiar things, without the burden of constant hospital visits. The heart of hospice is a good starting point if your family is trying to understand what that actually looks like day to day.
For families in Monterey County facing these decisions, the question isn’t usually whether to pursue palliative or hospice care — it’s when to ask. Asking earlier, before a crisis, leaves families with far more choices.
Skilled Home Health vs. Palliative Care vs. Hospice: A Quick Comparison
These three types of home-based care often get confused with each other. Here’s how they differ in purpose, timing, and coverage.
| Type of Care | Who It’s For | Medicare Coverage |
|---|---|---|
| Skilled Home Health | People recovering from illness, surgery, or managing a chronic condition who need clinical care at home | Covered when physician certifies homebound status and skilled need |
| Palliative Care | People with serious illness at any stage who need symptom management and support alongside other treatment | Partially covered; depends on services and plan — ask your care coordinator |
| Hospice Care | People with a terminal diagnosis choosing comfort-focused care over curative treatment | Fully covered under Medicare Hospice Benefit; also covered by most Medi-Cal plans |
The Practical Side: Safety, Family Roles, and What Families Often Miss
Even with excellent medical support in place, staying home requires some honest planning around the physical environment and family capacity.
In Monterey County, where a significant portion of the housing stock predates modern accessibility standards, a home safety assessment is often the most practical first step. Occupational Therapists who provide home health can evaluate a living space and recommend specific changes — not just grab bars, but lighting, furniture placement, and how to set up a bed or bathroom to reduce fall risk.
Falls are the leading cause of hospitalization for older adults in California, and many happen in the first few weeks after someone comes home from a hospital stay. That window — when someone is weaker than usual, on new medications, in familiar surroundings that suddenly feel less manageable — is exactly when skilled nursing care in Monterey can make the difference between a safe recovery and a return trip to the ER.
Family members also need to be honest about what they can sustain. Adult children in their 50s and 60s who are managing their own work schedules, health, and households are often doing more than they can carry long-term. A Medical Social Worker can help families map out what realistic support looks like — and where gaps exist — without judgment.
A few things families consistently underestimate:
- Medication complexity — managing 8 to 12 prescriptions at home is not straightforward, and errors are common
- Nighttime safety — most falls happen at night, when no one is watching
- Caregiver fatigue — family members burning out quietly, months before they’ll admit it
- The gap after discharge — hospitals discharge patients quickly; recovery happens at home, often with less support than families expect
Frequently Asked Questions About Aging at Home in Monterey County
How do we know if my parent actually qualifies for Medicare-covered home health?
A physician needs to certify two things: that your parent is homebound (meaning leaving the home requires considerable effort) and that they need a skilled service — nursing, physical therapy, occupational therapy, or speech therapy. If both conditions are met, Medicare Part A or Part B typically covers the cost. A care coordinator can help you determine eligibility based on your parent’s specific situation.
What’s the difference between a home health aide and a Registered Nurse visiting at home?
A home health aide helps with personal care — bathing, dressing, light tasks. A Registered Nurse provides clinical care: wound assessment, medication management, disease monitoring, and coordination with physicians. Both can visit the home, but they serve entirely different functions. Medicare covers skilled nursing visits; it does not cover personal aide services.
Can my parent receive palliative care and still continue cancer treatment or other curative care?
Yes. This is one of the most common misconceptions about palliative care. It is not an alternative to treatment — it runs alongside it. A patient can be receiving chemotherapy or dialysis and still have a palliative care team supporting symptom management and care planning at home.
How far in advance should families start thinking about hospice?
Most families say they waited too long. Hospice care can begin when a physician estimates a prognosis of six months or less if the illness follows its expected course. Calling earlier — even to ask questions — gives families more time to plan and more time to benefit from the support. There’s no commitment required from an initial conversation.
Does VNA serve areas outside Monterey, like Hollister or King City?
Yes. Central Coast VNA & Hospice serves all of Monterey County — including King City, Salinas, and the Monterey Peninsula — as well as San Benito County (including Hollister), and parts of Santa Cruz County and South Santa Clara County. If you’re unsure whether your address falls within the service area, calling 831-372-6668 is the quickest way to find out.
Have Questions About What Support Is Available?
Families across Monterey County — in Salinas, Carmel, Pacific Grove, King City, and Hollister — have been calling Central Coast VNA & Hospice with exactly the questions this article covers for more than 70 years. If you’re trying to figure out what kind of help your loved one qualifies for, or just want to talk through what the options look like, a care coordinator is available to help without any pressure. Call 831-372-6668 or visit ccvna.com to start the conversation.