Direct Answer: Home health supports recovery or disease management. Hospice is comfort-focused care when treatment is no longer the goal. Palliative care fits anywhere in between and is often the missing option families don’t know to ask about.
One of the most common calls families make to a home health agency goes something like this: a loved one is being discharged from Salinas Valley Health or Community Hospital of the Monterey Peninsula, and the family has 48 hours to figure out what happens next. They’ve heard the words home health, palliative care, and hospice — sometimes in the same conversation — and they’re not sure which one applies or whether their loved one even qualifies.
That confusion is completely understandable. These three types of care are genuinely different — different goals, different eligibility rules, different teams involved — but from the outside, they can sound like variations of the same thing. And when a discharge planner is waiting on a decision, there’s rarely time to sort it out quietly.
This article explains how these three options actually differ, who qualifies for each, and — critically — how a patient can move between them as their needs change. If you’re making this decision for someone in Monterey County, Salinas, Pacific Grove, King City, or anywhere else on the Central Coast, this is meant to give you a clear picture before you talk to anyone.
What Home Health Actually Is — and Who It’s For
Home health is medical care delivered in the home for patients who are still working toward a goal — recovering from surgery, managing a worsening chronic condition, or regaining function after a hospital stay. The word that matters here is goal. Home health is built around measurable progress.
To qualify under Medicare, a patient generally needs to meet two criteria:
- They must be homebound, meaning leaving home requires significant effort or assistance
- They must need skilled care — services that only a licensed clinician can provide, not just help with daily tasks
What that looks like in practice is a care team that might include a Registered Nurse managing medications and monitoring for complications, a Physical Therapist rebuilding strength and mobility after a hip replacement, an Occupational Therapist helping someone adapt their home routine, or a Speech Therapist addressing swallowing difficulties after a stroke. A Medical Social Worker may also be involved to connect the family with community resources and support.
One family from Pacific Grove described the moment their mother came home from rehab: a nurse arrived first to assess her needs, then a physical therapist came weekly to work through an individualized exercise plan, and a medical social worker helped them sort out her Medicaid paperwork from another state. That combination — not just nursing, but a full team with specific roles — is what home health actually looks like when it’s working.
For more on what happens during those visits, What Does a Skilled Nurse Actually Do on a Home Visit? explains the details in plain terms. And if you’re navigating a discharge right now, What Families Often Miss When Planning a Hospital Discharge to Home is worth reading before you finalize anything.
What Hospice Is — and What It Isn’t
Hospice represents a different philosophy entirely. It’s not a lower level of home health — it’s a different choice about what care is for.
When a patient and their physician agree that curative or life-prolonging treatment is no longer the goal, and a physician certifies a prognosis of six months or less if the illness follows its expected course, hospice becomes available. At that point, Medicare’s hospice benefit covers the full scope of comfort-focused care in the home.
What that team looks like:
- Hospice Registered Nurses managing pain and symptoms, available around the clock
- Hospice Aides assisting with personal care and daily comfort
- Medical Social Workers supporting the patient and family with practical and emotional needs
- Chaplains providing spiritual care — regardless of religious background
- Bereavement Specialists who stay connected with families after the patient’s passing
- Volunteers who provide companionship and respite
One reviewer described receiving care for a parent in a terminal situation: “They don’t just show up to work everyday for us in need — they care for our loved ones that are in need of support through the very hard times life brings.”
A few things families often get wrong about hospice: it doesn’t mean giving up hope, it doesn’t mean the patient dies sooner, and — importantly — it’s a choice the patient can reverse. If someone on hospice decides they want to pursue treatment again, they can leave hospice and return to curative care. That flexibility rarely gets communicated clearly, and it changes how many families approach the conversation.
For a deeper look at what this decision actually feels like, How Families Describe the Moment They Chose Hospice reflects honest accounts from people who’ve been there.
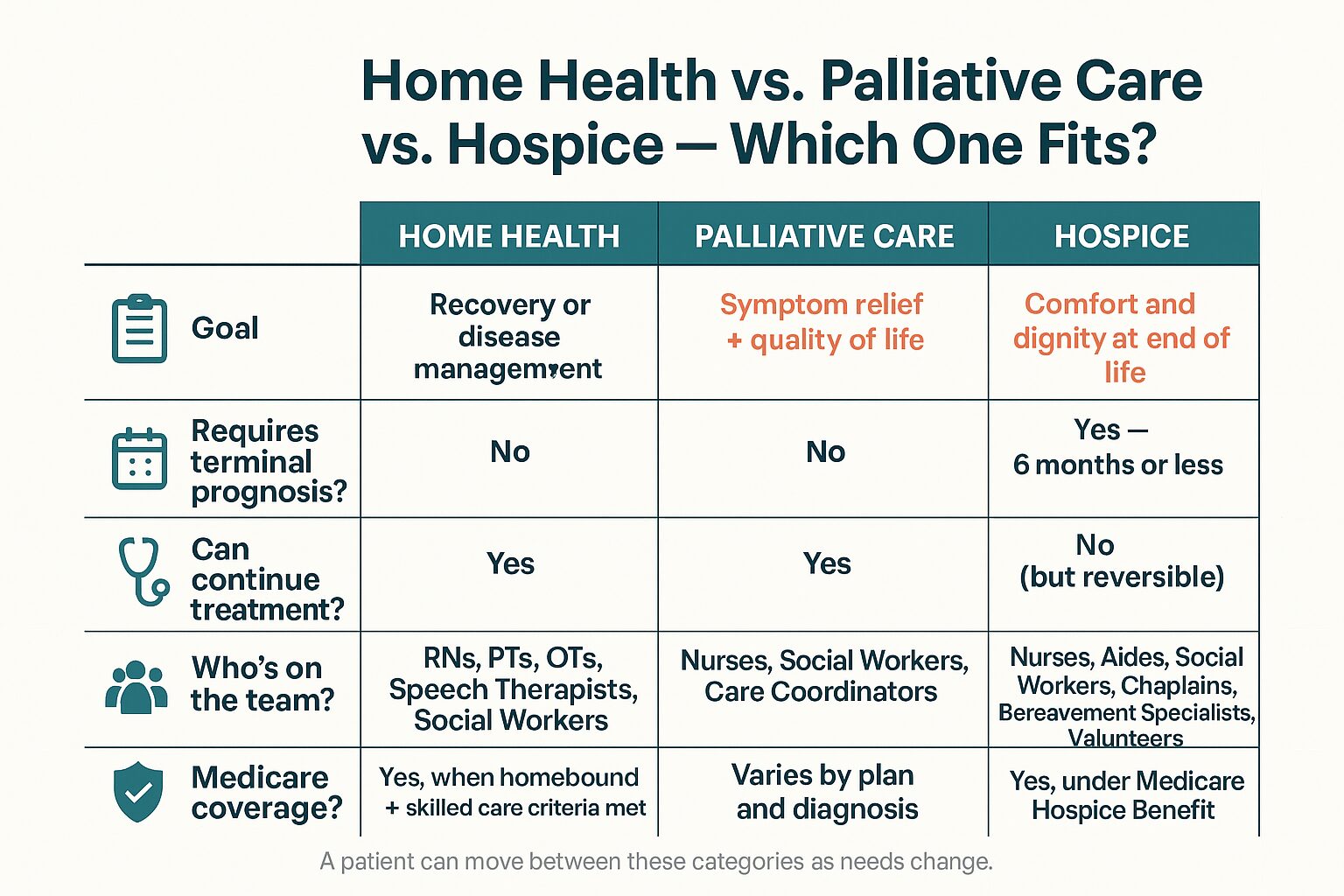
The Three Paths: Home Health, Palliative Care, and Hospice
This comparison shows how home health, palliative care, and hospice differ across the dimensions families ask about most.

Palliative Care: The Option Most Families Have Never Heard Of
If home health is about recovery and hospice is about comfort at end of life, palliative care sits in a space most families don’t realize exists.
Palliative care is available at any stage of a serious illness — even alongside active treatment. It does not require a terminal diagnosis. A person receiving chemotherapy, managing a progressive neurological condition like Parkinson’s, or living with advanced heart failure can all qualify. The focus is on managing symptoms, improving quality of life, supporting the family, and helping everyone involved make informed decisions about what comes next.
In real terms, palliative care might look like:
- A nurse practitioner or physician working alongside the treating doctor to control pain and fatigue
- A medical social worker helping the family understand their options and anticipate what’s ahead
- Emotional and psychosocial support for the patient and for family members carrying the weight of caregiving
- Care planning conversations that happen before a crisis forces a rushed decision
One caller navigating a Parkinson’s diagnosis for her husband didn’t know whether he would qualify for any services at all. Palliative care was the answer — not home health, not hospice — and it’s the category most likely to be missing from the conversation families are having right now.
For a full explanation of what palliative care actually involves, Palliative Care Meaning: A 2026 Guide to Family Support is a good place to start. And What “Comfort-Focused Care” Really Means — and When to Ask About It addresses the language families often encounter without a clear explanation.
Can a Patient Move Between These Categories?
This is one of the most important questions families ask — and the answer is almost always yes. Here’s how those transitions typically work.
| Starting Point | Transition | What Makes It Possible |
|---|---|---|
| Home Health | → Palliative Care | Illness progresses; curative treatment continues but symptom burden increases |
| Home Health | → Hospice | Patient and physician agree comfort is now the goal; prognosis of 6 months or less |
| Palliative Care | → Hospice | Patient elects to stop curative treatment; palliative team often helps facilitate |
| Hospice | → Home Health or Curative Treatment | Patient decides to resume treatment; hospice is revoked; Medicare covers new plan |
| Hospice | Continued beyond 6 months | Patient outlives initial prognosis; hospice continues with physician recertification |
How Families in Monterey County Are Actually Making This Decision
In practice, the families calling with these questions are rarely sitting calmly with time to research. More often, someone is being discharged from a hospital in Marina or Carmel, a specialist has said something that changed everything, or a parent who was managing fine last month is no longer managing at all.
Several patterns come up repeatedly among families navigating this on the Central Coast:
- Families with a loved one in a skilled nursing facility — places like Canterbury Woods in Pacific Grove — trying to understand what home health looks like once their parent returns home
- Adult children managing a parent’s medications who realize the complexity has exceeded what they can safely handle alone
- Spouses of patients with dementia, Parkinson’s, or cancer who have been carrying everything themselves and aren’t sure where to draw the line
What changes the conversation for many of these families is learning that the care team is larger than they assumed. Many callers are surprised to find out that physical therapists, occupational therapists, medical social workers, and chaplains are part of the picture — not just nurses. When a discharge planner or agency representative describes that full team clearly and early, it often resolves the hesitation.
If you’re in that position right now — caring for an aging parent and trying to figure out when you’ve reached the edge of what you can do alone — When Caring for an Aging Parent Becomes More Than You Can Do Alone addresses that experience directly.
Frequently Asked Questions About Home Health vs. Hospice
My mother’s doctor mentioned home health after her surgery. Does she automatically qualify?
Not automatically — but most post-surgical patients do qualify if they meet two conditions: they’re homebound (meaning leaving home takes considerable effort), and they need skilled care like nursing, physical therapy, or wound care. A physician order is required, and an agency will do an initial evaluation to confirm eligibility before services begin.
Does choosing hospice mean we’re giving up?
No. Hospice is a choice about what kind of care fits best at a particular moment — not a surrender. Many families describe it as the first time their loved one felt genuinely comfortable. And it’s worth knowing that hospice is revocable: if a patient wants to return to curative treatment, they can. The decision isn’t permanent.
Can someone be on hospice and still live at home?
Yes — that’s actually the most common arrangement. Hospice care is designed to be delivered in the home, and the team — nurses, aides, chaplains, social workers, and volunteers — comes to the patient. A patient doesn’t need to move to a facility to receive hospice.
We’re not sure if we’re at the hospice stage yet. What’s in between?
Palliative care is the answer most families don’t know to ask about. It’s available at any stage of serious illness, alongside whatever treatment is already happening. It doesn’t require a terminal prognosis. If your loved one is dealing with significant symptoms, medication complexity, or emotional strain — and they’re still pursuing treatment — palliative care may fit right now.
Does Medicare cover all of this?
Medicare covers home health when the patient is homebound and needs skilled care, ordered by a physician. It covers hospice fully under the Medicare Hospice Benefit when a physician certifies a prognosis of six months or less and the patient elects comfort-focused care. Palliative care coverage varies — it depends on the patient’s diagnosis, their Medicare plan, and how services are structured. VNA accepts Medicare, Medi-Cal, and Veterans benefits; a care coordinator can walk through what applies to your loved one’s specific situation.
Can a patient receive home health in Salinas or King City, not just on the Monterey Peninsula?
Yes. Central Coast VNA & Hospice serves all of Monterey County — including Salinas, King City, the Monterey Peninsula, and surrounding communities — as well as San Benito County, South Santa Clara County, and parts of the region beyond. Geographic coverage is worth confirming when you call, especially for more rural areas.
Still Not Sure Which One Fits?
That’s exactly the kind of question a care coordinator at Central Coast VNA & Hospice can help sort out — without pressure, and without requiring you to have it figured out first. VNA has been serving families across Monterey County, Salinas, the Monterey Peninsula, and the broader Central Coast since 1951, and this conversation is one they have every day. You can reach them at 831-372-6668 or visit ccvna.com to learn more about the options available to your family right now.