Direct Answer: Families who plan early experience less conflict, fewer emergency decisions, and more meaningful time together. Starting doesn’t mean accepting death is near — it means being ready if it comes.
Most families on the Central Coast don’t avoid end-of-life planning because they don’t care. They avoid it because starting feels like admitting something is already over.
But that belief — that planning means giving up — is exactly what leads to the hardest moments: a family disagreeing in a hospital hallway at midnight, a loved one unable to speak for themselves, a physician asking questions no one prepared to answer. Across Monterey County, these situations play out regularly, and almost all of them were preventable.
This article covers what end-of-life planning actually includes, why earlier is genuinely better, and what California’s legal documents mean for your family — explained in plain terms, without pressure.
What End-of-Life Planning Actually Covers (It’s More Than a Document)
When most people hear “end-of-life planning,” they picture a single piece of paperwork. The reality is more like a set of conversations — some legal, some deeply personal — that together give your family a map when things get hard.
A complete plan typically addresses:
- Who makes decisions if you can’t speak for yourself
- What treatments you want — and which ones you don’t
- Where you want to be — home, a facility, or somewhere specific in your community
- Pain and symptom preferences — how aggressively you want discomfort managed
- Spiritual and cultural wishes — what matters at the end in terms of faith, ritual, and presence
- What your family needs to know about finances, accounts, and practical logistics
Most families get to one or two of these. The rest become crises — not because anyone failed, but because no one knew the conversation needed to happen.
For families in Salinas, Pacific Grove, King City, or anywhere across Monterey County, what families in Monterey wish they’d known sooner about home care reflects a recurring theme: the questions people wish they’d asked earlier.
California’s Three Advance Directive Documents — and What Each One Does
California recognizes three distinct legal documents for end-of-life planning. They’re not interchangeable, and each one serves a different function. Understanding which is which — and who needs to have a copy — is one of the most practical things a family can do.
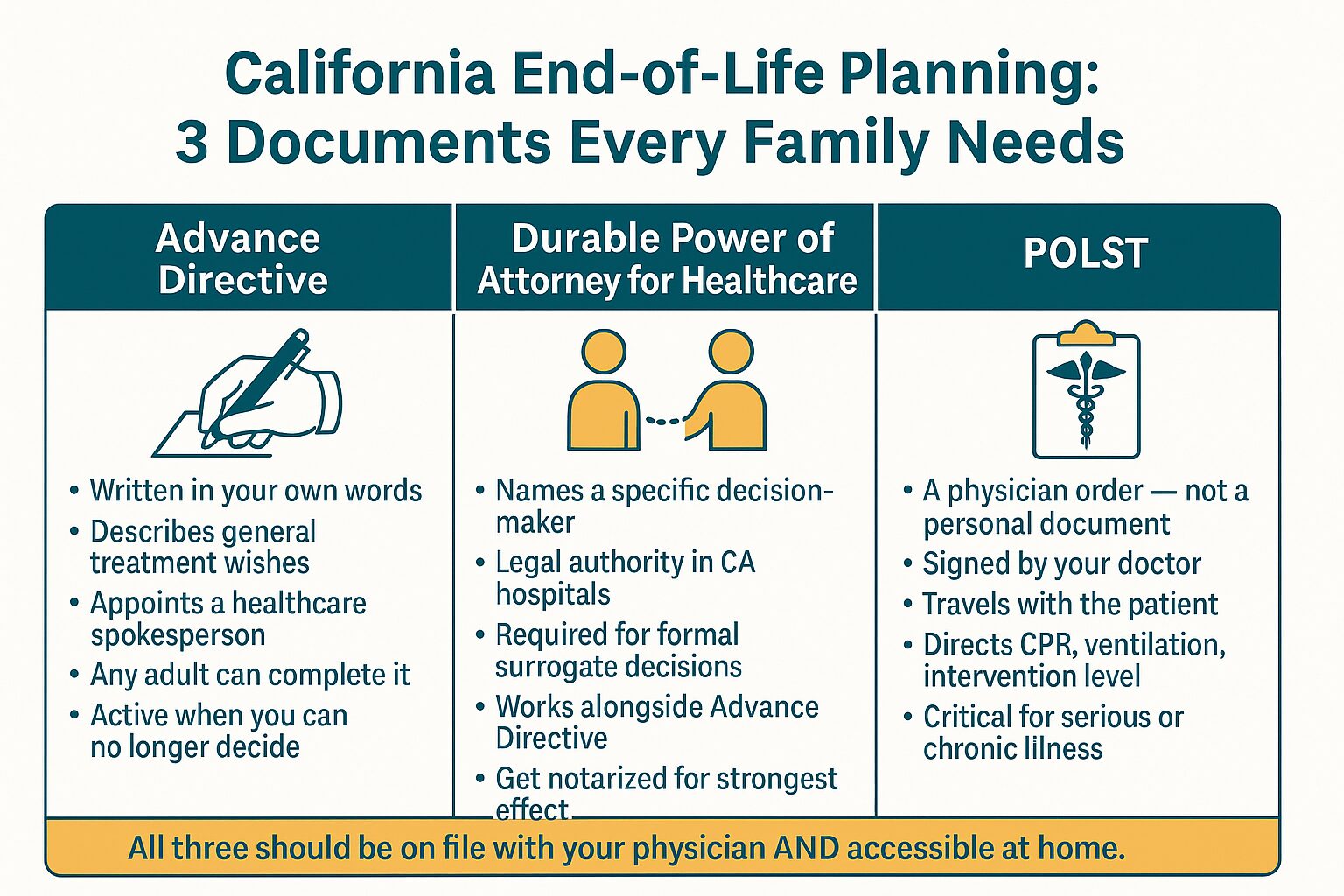
1. Advance Directive (also called a Healthcare Directive)
This is the broadest document. It lets you describe your general wishes for medical treatment and designate someone to speak for you. It’s written in your own words and becomes active when a physician determines you can no longer make decisions yourself. Any adult in California can complete one without an attorney.
2. Durable Power of Attorney for Healthcare (DPAHC)
This document formally appoints a specific person — your healthcare agent — to make medical decisions on your behalf. It has legal weight in California hospitals and medical settings. Without it, a hospital may default to its own protocol for surrogate decision-making, which may not reflect what you’d want.
3. POLST (Physician Orders for Life-Sustaining Treatment)
This is not an advance directive — it’s a medical order, signed by a physician. It travels with a patient and gives emergency responders and medical staff specific, actionable instructions: whether to attempt CPR, whether to use mechanical ventilation, what level of intervention you want. A POLST is especially important for people with serious or chronic illness who may need emergency care at home.
All three documents should be:
– On file with your primary physician
– Accessible to your designated decision-maker
– Kept somewhere findable at home — not locked in a safe deposit box
If you’re caring for an aging parent in Hollister, Seaside, or anywhere across Monterey County, having all three in order — and copies distributed — means a physician, nurse, or paramedic will know exactly what your family wants.
California’s Three Advance Directive Documents at a Glance
This infographic breaks down the three documents California families need, what each one covers, and who should have a copy.

Why Families Wait — and What Research and Experience Actually Show
The most common reason families delay isn’t avoidance. It’s a specific belief: that starting the conversation means accepting that death is close.
But families who plan early consistently report the opposite experience. Less conflict. Fewer emergency decisions. More time spent actually present with their loved one instead of managing a crisis.
One reason early planning changes the experience is that it removes a particular kind of stress — the stress of not knowing what the person would want. When a Registered Nurse or Medical Social Worker visits a patient at home and the family has already had these conversations, the clinical team can focus on care instead of spending precious time reconstructing preferences from scratch.
For families weighing whether a loved one still needs curative treatment or might benefit from a different kind of support, what comfort-focused care really means — and when to ask about it is worth reading before those conversations happen in a hospital setting.
Palliative Care Isn’t an End — It’s a Different Kind of Beginning
One of the most persistent misunderstandings in end-of-life planning is the belief that seeking additional support means stopping treatment. It doesn’t.
Palliative care is specifically designed to run alongside curative treatment. A patient in Monterey County who is still pursuing chemotherapy, cardiac intervention, or aggressive management of a chronic condition can also have a palliative care team providing:
- Symptom management — pain, fatigue, nausea, breathlessness
- Emotional and psychosocial support for both patient and family
- Care coordination with treating physicians
- Honest, unhurried conversations about what the patient actually wants
This is not an all-or-nothing choice. The framing that palliative care means “giving up” keeps many families from seeking earlier support — and that delay often means more suffering, not less.
In April 2024, California passed AB 1005, which now requires hospitals and Medi-Cal managed care plans to inform terminally ill patients about in-home supportive services and palliative options. Patients with serious illness have more locally available options than they’re typically told about during a hospital stay — and knowing to ask is half the work.
For a deeper look at what this kind of care involves, the advanced guide to palliative care in Monterey at home explains the practical side in plain terms.
What Hospice Actually Includes — and When to Have the Conversation
Hospice care is one of the most misunderstood options in end-of-life planning — and one of the most underused, often because families wait until the very last weeks to ask about it.
Hospice is appropriate when a patient’s illness is no longer responding to curative treatment and the focus shifts to comfort and quality of life. In California, a patient generally qualifies for the Medicare Hospice Benefit when two physicians certify a prognosis of six months or less if the illness runs its natural course.
But hospice isn’t just pain management. A full interdisciplinary team typically includes:
- Registered Nurses and Licensed Vocational Nurses for symptom management and clinical monitoring
- Medical Social Workers for care planning and family support
- Hospice Aides for personal care
- Chaplains for spiritual care, regardless of faith background
- Bereavement Specialists who continue supporting the family after the patient passes
- Volunteers who provide companionship and respite
Medicare and Medi-Cal both cover hospice services when eligibility criteria are met. Veterans benefits also apply for qualifying patients.
Many families describe the decision to ask about hospice as the moment things finally felt less chaotic — not more. How families describe the moment they chose hospice captures that experience directly, in their own words.
Palliative Care vs. Hospice Care: Key Differences
Families often confuse these two types of care. This table breaks down the main distinctions so you know what you’re asking about — and when each applies.
| Palliative Care | Hospice Care | |
|---|---|---|
| Curative treatment continues? | Yes — runs alongside treatment | No — focus shifts to comfort only |
| Eligibility | Any serious illness, any stage | Prognosis of 6 months or less (if illness runs its course) |
| Care team | Nurses, therapists, social workers, chaplains | Nurses, aides, social workers, chaplains, bereavement specialists, volunteers |
| Medicare/Medi-Cal coverage | Covered under certain plans; varies | Fully covered under Medicare Hospice Benefit and Medi-Cal when eligible |
| Where care happens | Home, clinic, or hospital | Primarily at home or in a home-like setting |
| Goal | Symptom relief, care coordination, quality of life | Comfort, dignity, and family support through end of life |
What Grief Looks Like Before and After — and Why Bereavement Support Belongs in the Plan
End-of-life planning doesn’t end when a patient passes. Families who’ve been through a serious illness often carry grief that started long before the death — grief for the person they’re watching change, for the life that got interrupted, for the decisions they’re still carrying.
Anticipatory grief is real and common, especially for adult children who’ve become primary decision-makers for an aging parent. Having a Medical Social Worker or Bereavement Specialist as part of the care team — not just after the death, but during the illness — gives families a real outlet.
Bereavement support that begins before a loss tends to make the months afterward less isolating. For families in the Seaside, Hollister, or Salinas areas who find themselves without a nearby support group, grief doesn’t follow a schedule — what support actually helps is a practical starting point.
Frequently Asked Questions About End-of-Life Planning
Does starting end-of-life planning mean we’re giving up?
No — and this is the most important thing to understand. Planning early doesn’t signal that death is close. It means that if something happens suddenly, your family doesn’t have to make irreversible decisions under pressure. Families who plan earliest consistently report more meaningful time with their loved one, not less.
What’s the difference between an Advance Directive and a POLST?
An Advance Directive is a personal document that describes your general wishes and names someone to speak for you. A POLST is a physician-signed medical order that travels with you and gives emergency responders specific instructions — CPR, ventilation, level of intervention. Both are important, and they serve different situations. If your loved one has a serious or chronic illness, they likely need both.
Can someone still receive palliative care if they’re pursuing curative treatment?
Yes. Palliative care runs alongside treatment — it doesn’t replace it. A patient who is still actively treating cancer, heart disease, or another serious condition can simultaneously receive symptom management, emotional support, and care coordination from a palliative care team. California’s AB 1005 (2024) now requires hospitals and Medi-Cal plans to tell seriously ill patients about these options.
Does Medicare cover hospice care at home?
Medicare fully covers the hospice benefit when two physicians certify that a patient’s prognosis is six months or less if the illness runs its natural course, and when the patient elects to focus on comfort rather than curative treatment. Medi-Cal and Veterans benefits also cover hospice under qualifying circumstances. Coverage typically includes nursing visits, medications related to the terminal diagnosis, aide services, chaplain visits, and bereavement support for the family.
Who should have copies of our end-of-life planning documents?
At minimum: your primary physician, your designated healthcare agent (the person named in your Durable Power of Attorney for Healthcare), and a family member who knows where to find the originals quickly. Your POLST should be posted somewhere visible at home — on the refrigerator is the standard recommendation — so that emergency responders can find it fast. Locked away in a safe deposit box is the one place it will not be useful when it’s needed most.
How do we start this conversation with a parent who doesn’t want to talk about it?
Start smaller than you think you need to. Instead of ‘let’s talk about what happens when you die,’ try ‘I want to make sure I know what’s important to you if something ever happened.’ Most people have strong feelings about where they want to be cared for and what they don’t want done to them medically — they just haven’t been asked. A Medical Social Worker can also help facilitate these conversations, particularly when family dynamics make them feel loaded.
Questions About Where to Start?
Central Coast VNA & Hospice has been supporting families across Monterey County, Salinas, King City, Hollister, and the surrounding Central Coast since 1951 — including families navigating these exact conversations for the first time. If you’re not sure what documents your family needs, whether a loved one might qualify for palliative or hospice care, or just want to talk through the options, a care coordinator can help you find your footing. Call 831-372-6668 or visit ccvna.com to learn more.